

Predictive efficacy of combined tumor markers and gastrin for recurrence after endoscopic submucosal dissection in early gastric cancer patients
- PMID: 38883344
- PMCID: PMC11170613
- DOI: 10.62347/VOTO5604
Predictive efficacy of combined tumor markers and gastrin for recurrence after endoscopic submucosal dissection in early gastric cancer patients
Abstract
Objective: This study aims to evaluate the predictive value of tumor markers combined with gastrin for tumor recurrence after endoscopic submucosal dissection (ESD) in patients with early gastric cancer.
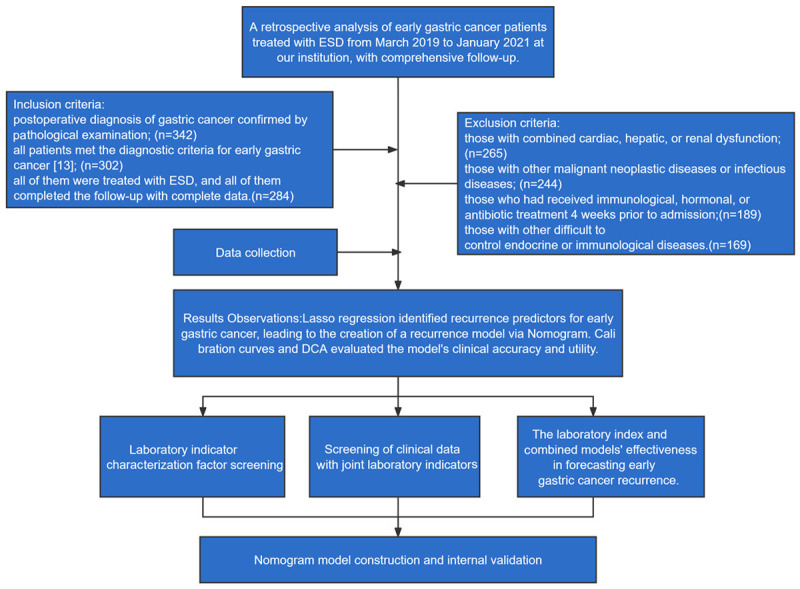
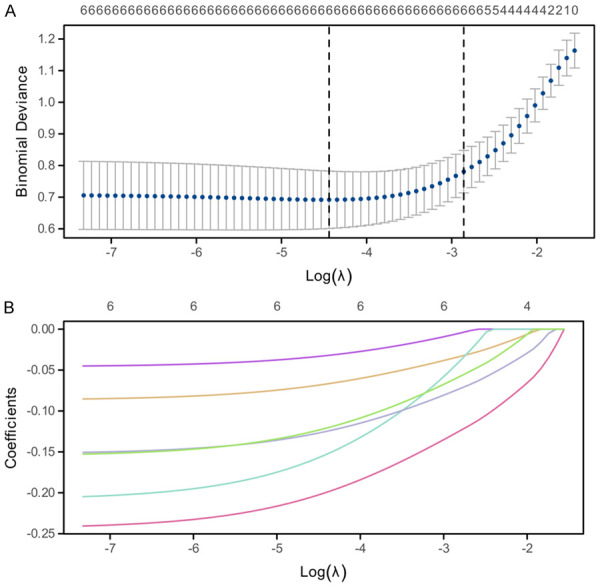
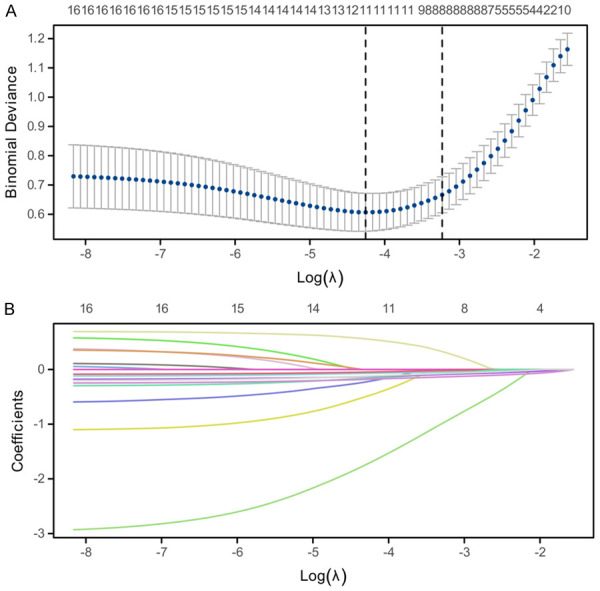
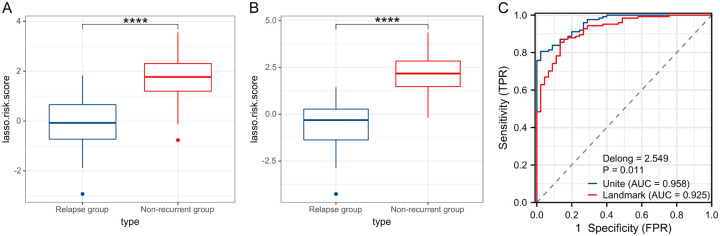
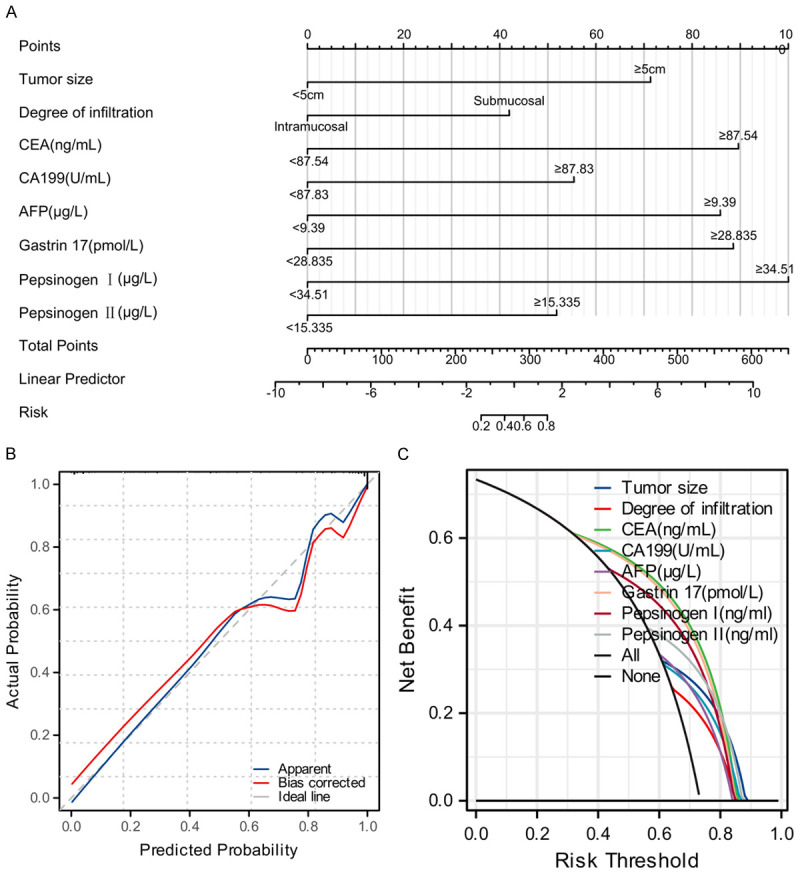
Methods: The clinicopathological data of 169 patients with early gastric cancer treated with ESD between March 2019 and January 2021 were retrospectively analyzed. The patients were divided into a relapse group (n=45) and a non-recurrence group (n=124). Clinical data such as carcinoembryonic antigen (CEA), cancer antigen 19-9 (CA19-9), alpha-fetoprotein (AFP), gastrin 17, pepsinogen I and pepsinogen II, as well as tumor size and degree of infiltration were examined to construct a recurrence prediction model using lasso regression.
Results: The comprehensive model showed superior predictive power (AUC=0.958, C-index=0.966) over biomarker-only models (AUC=0.925), indicating a significant improvement in the prediction of recurrence risk. Decision curve analysis confirmed the clinical utility of the model with a maximum net benefit of 73.37%. Key indicators such as CEA, CA19-9, AFP, gastrin 17 and pepsinogens I and II were statistically significant in predicting recurrence with P values < 0.01.
Conclusion: The comprehensive model combining tumor markers with clinical data provides a more accurate and clinically valuable tool for predicting recurrence in early gastric cancer patients after ESD. This approach facilitates personalized risk assessment and may significantly improve prognostic management, emphasizing the importance of a multifaceted strategy in the management of early gastric cancer.
Keywords: Tumor marker; early gastric cancer; endoscopic submucosal dissection; gastrin; prediction; recurrence.
AJTR Copyright © 2024.
Conflict of interest statement
None.
Figures
Similar articles
-
A Proton Pump Inhibitor Independently Elevates Gastrin Levels as a Marker for Metachronous Gastric Cancer After Endoscopic Submucosal Dissection.J Clin Med. 2024 Nov 3;13(21):6599. doi: 10.3390/jcm13216599. J Clin Med. 2024. PMID: 39518740 Free PMC article.
-
Early detection of recurrence after endoscopic treatment for early gastric cancer.Scand J Gastroenterol. 2009;44(9):1109-14. doi: 10.1080/00365520903121701. Scand J Gastroenterol. 2009. PMID: 19593687
-
Construction and analysis of an ulcer risk prediction model after endoscopic submucosal dissection for early gastric cancer.World J Gastrointest Oncol. 2022 Sep 15;14(9):1823-1832. doi: 10.4251/wjgo.v14.i9.1823. World J Gastrointest Oncol. 2022. PMID: 36187385 Free PMC article.
-
Comparison of CEA and CA19-9 as a predictive factor for recurrence after curative gastrectomy in gastric cancer.BMC Surg. 2022 Jun 3;22(1):213. doi: 10.1186/s12893-022-01667-z. BMC Surg. 2022. PMID: 35655198 Free PMC article. Review.
-
AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States.Clin Gastroenterol Hepatol. 2019 Jan;17(1):16-25.e1. doi: 10.1016/j.cgh.2018.07.041. Epub 2018 Aug 2. Clin Gastroenterol Hepatol. 2019. PMID: 30077787 Review.
References
-
- Zong L, Abe M, Seto Y, Ji J. The challenge of screening for early gastric cancer in China. Lancet. 2016;388:2606. - PubMed
-
- Wender RC, Brawley OW, Fedewa SA, Gansler T, Smith RA. A blueprint for cancer screening and early detection: advancing screening’s contribution to cancer control. CA Cancer J Clin. 2019;69:50–79. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous