

How Reliable Is Endoscopic Scoring of Postoperative Recurrence in Crohn Disease?: A Systematic Review and Meta-Analysis
- PMID: 38883962
- PMCID: PMC11175939
- DOI: 10.1097/AS9.0000000000000397
How Reliable Is Endoscopic Scoring of Postoperative Recurrence in Crohn Disease?: A Systematic Review and Meta-Analysis
Abstract
Objective: Guidelines advise to perform endoscopic surveillance following ileocolic resection (ICR) in Crohn disease (CD) for timely diagnosis of recurrence. This study aims to assess the variation in endoscopic recurrence (ER) rates in patients after ICR for CD using the most commonly used classification systems, the Rutgeerts score (RS) and modified Rutgeerts score (mRS) classifications.
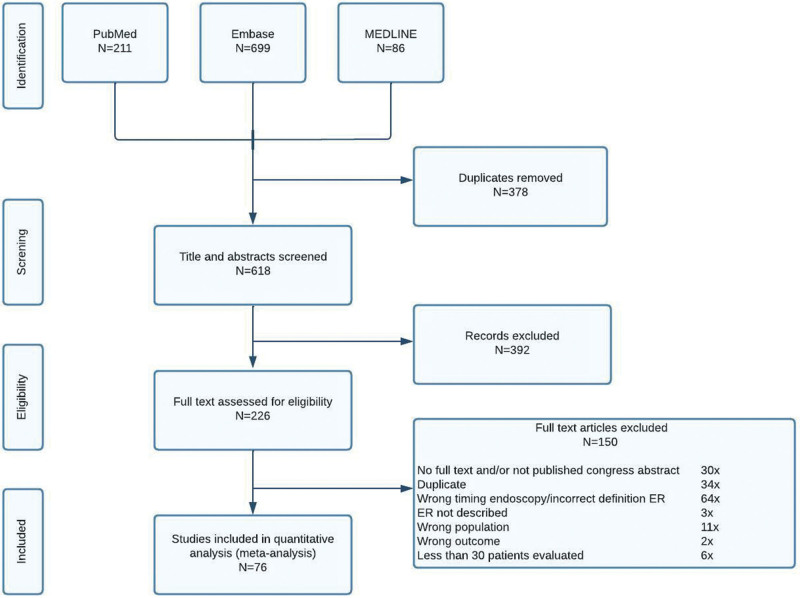
Methods: A systematic literature search using MEDLINE, Embase, and the Cochrane Library was performed. Randomized controlled trials and cohort studies describing ER < 12 months after an ICR for CD were included. Animal studies, reviews, case reports (<30 included patients), pediatric studies, and letters were excluded. The Newcastle-Ottawa Quality Assessment Scale and Cochrane Collaboration's tool were used to assess risk of bias. Main outcome was the range of ER rates within 12 months postoperatively, defined as RS ≥ i2 and/or mRS ≥ i2b. A proportional meta-analysis was performed. The final search was performed on January 4, 2022. The study was registered at PROSPERO, CRD42022363208.
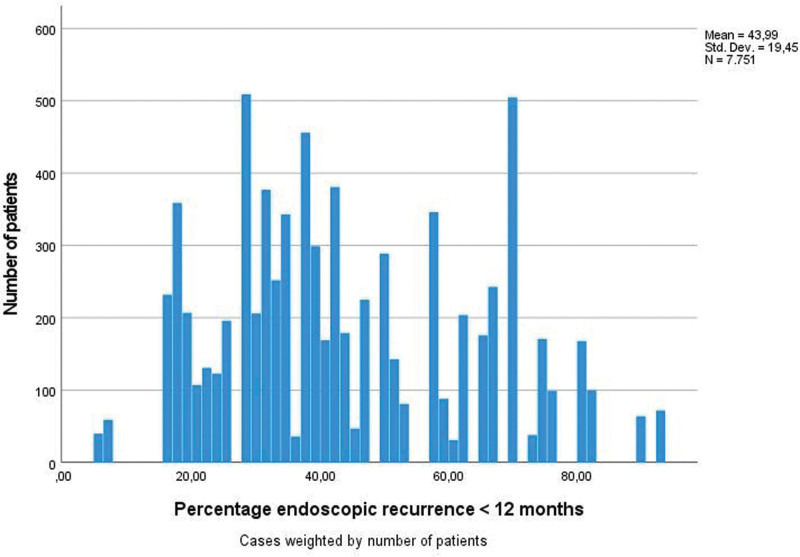
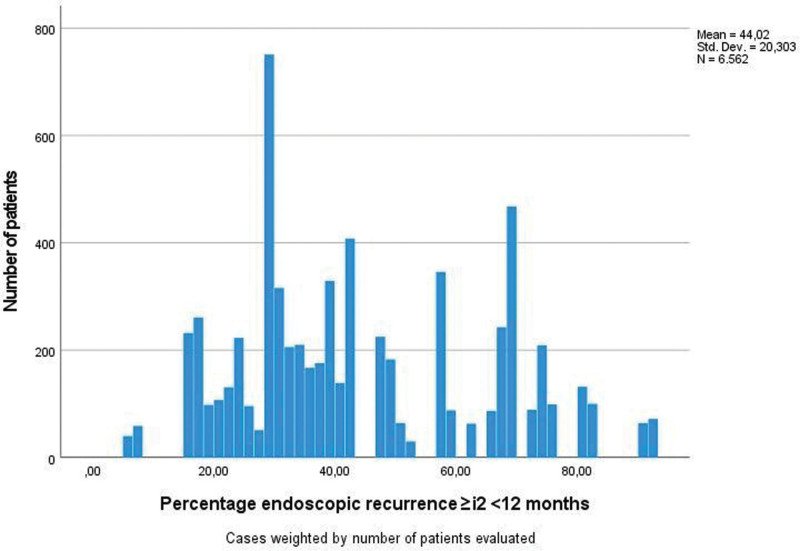
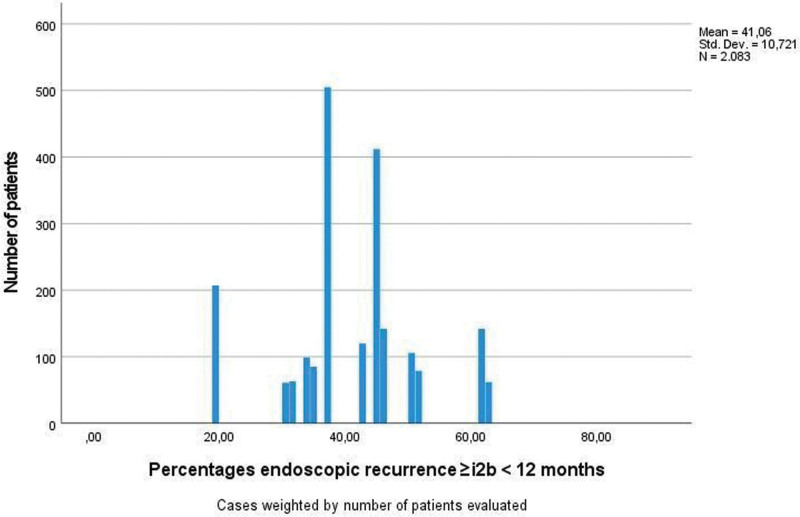
Results: Seventy-six studies comprising 7751 patients were included. The weighted mean of ER rates in all included studies was 44.0% (95% confidence interval, 43.56-44.43). The overall range was 5.0% to 93.0% [interquartile range (IQR), 29.2-59.0]. The weighted means for RS and mRS were 44.0% and 41.1%, respectively. The variation in ER rates for RS and mRS were 5.0% to 93.0% (IQR, 29.0-59.5) and 19.8% to 62.9% (IQR, 37.3-46.5), respectively. Within studies reporting both RS and mRS, the weighted means for ER were 61.3% and 40.6%, respectively.
Conclusions: This study demonstrates a major variation in ER rates after ICR for CD, suggesting a high likelihood of inadequate diagnosis of disease recurrence, with potentially impact on quality of life and health care consumption. Therefore, there is an important need to improve endoscopic scoring of recurrent disease.
Keywords: (modified) Rutgeerts score; Crohn disease; ileocolic resection; postoperative endoscopic recurrence.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures
Similar articles
-
Comparison of the Risk of Crohn's Disease Postoperative Recurrence Between Modified Rutgeerts Score i2a and i2b Categories: An Individual Patient Data Meta-analysis.J Crohns Colitis. 2023 Mar 18;17(2):269-276. doi: 10.1093/ecco-jcc/jjac137. J Crohns Colitis. 2023. PMID: 36124813 Free PMC article.
-
Correlation Between Calprotectin and Modified Rutgeerts Score.Inflamm Bowel Dis. 2016 Sep;22(9):2173-81. doi: 10.1097/MIB.0000000000000850. Inflamm Bowel Dis. 2016. PMID: 27482974
-
Differential risk of disease progression between isolated anastomotic ulcers and mild ileal recurrence after ileocolonic resection in patients with Crohn's disease.Gastrointest Endosc. 2019 Aug;90(2):269-275. doi: 10.1016/j.gie.2019.01.029. Epub 2019 Feb 6. Gastrointest Endosc. 2019. PMID: 30738034 Free PMC article.
-
Preventing Recurrence of Crohn's Disease Post-Ileocaecal Surgery in Paediatric Patients: A Therapy Guide Based on Systematic Review of the Evidence.Paediatr Drugs. 2024 Nov;26(6):659-672. doi: 10.1007/s40272-024-00650-w. Epub 2024 Aug 31. Paediatr Drugs. 2024. PMID: 39215954
-
Colonoscopy-guided therapy for the prevention of post-operative recurrence of Crohn's disease.Cochrane Database Syst Rev. 2020 Aug 3;8(8):CD012328. doi: 10.1002/14651858.CD012328.pub2. Cochrane Database Syst Rev. 2020. PMID: 32746500 Free PMC article.
Cited by
-
Extended mesenteric resection reduces the rate of surgical recurrence in Crohn's disease: a systematic review and meta-analysis.Int J Colorectal Dis. 2025 Feb 25;40(1):51. doi: 10.1007/s00384-025-04845-6. Int J Colorectal Dis. 2025. PMID: 39998692 Free PMC article.
-
The Impact of Postoperative Prophylactic Medication on Long-Term Surgical, Severe Endoscopic and Endoscopic or Radiologic Recurrence Following Primary Ileocecal Resection in Patients With Crohn's Disease.Aliment Pharmacol Ther. 2025 Mar;61(6):1019-1031. doi: 10.1111/apt.18496. Epub 2025 Jan 24. Aliment Pharmacol Ther. 2025. PMID: 39856782 Free PMC article.
References
-
- Stevens TW, Haasnoot ML, D’Haens GR, et al. ; LIR!C study group. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn’s disease: retrospective long-term follow-up of the LIR!C trial. Lancet Gastroenterol Hepatol. 2020;5:900–907. - PubMed
-
- Ponsioen CY, de Groof EJ, Eshuis EJ, et al. ; LIR!C study group. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn’s disease: a randomised controlled, open-label, multicentre trial. Lancet Gastroenterol Hepatol. 2017;2:785–792. - PubMed
-
- Gionchetti P, Dignass A, Danese S, et al. ; ECCO. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: part 2: surgical management and special situations. J Crohns Colitis. 2017;11:135–149. - PubMed
-
- Rutgeerts P, Geboes K, Vantrappen G, et al. . Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990;99:956–963. - PubMed
-
- Buisson A, Chevaux JB, Allen PB, et al. . Review article: the natural history of postoperative Crohn’s disease recurrence. Aliment Pharmacol Ther. 2012;35:625–633. - PubMed
LinkOut - more resources
Full Text Sources
