

Type 2 Biomarkers and Their Clinical Implications in Bronchiectasis: A Prospective Cohort Study
- PMID: 38884647
- PMCID: PMC11427600
- DOI: 10.1007/s00408-024-00707-0
Type 2 Biomarkers and Their Clinical Implications in Bronchiectasis: A Prospective Cohort Study
Abstract
Purpose: Bronchiectasis is predominantly marked by neutrophilic inflammation. The relevance of type 2 biomarkers in disease severity and exacerbation risk is poorly understood. This study explores the clinical significance of these biomarkers in bronchiectasis patients.
Methods: In a cross-sectional cohort study, bronchiectasis patients, excluding those with asthma or allergic bronchopulmonary aspergillosis, underwent clinical and radiological evaluations. Bronchoalveolar lavage samples were analyzed for cytokines and microbiology. Blood eosinophil count (BEC), serum total immunoglobulin E (IgE), and fractional exhaled nitric oxide (FeNO) were measured during stable disease states. Positive type 2 biomarkers were defined by established thresholds for BEC, total IgE, and FeNO.
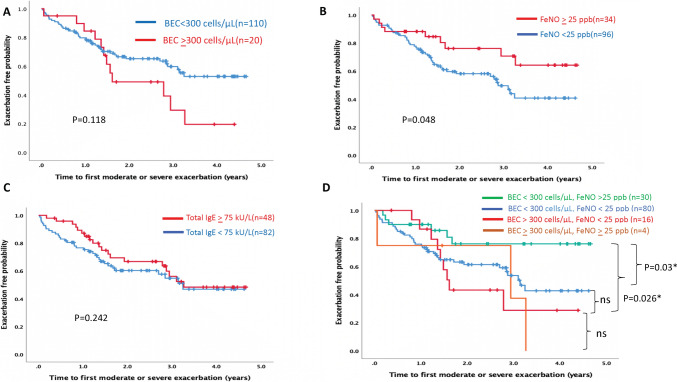
Results: Among 130 patients, 15.3% demonstrated BEC ≥ 300 cells/μL, 26.1% showed elevated FeNO ≥ 25 ppb, and 36.9% had high serum total IgE ≥ 75 kU/L. Approximately 60% had at least one positive type 2 biomarker. The impact on clinical characteristics and disease severity was variable, highlighting BEC and FeNO as reflective of different facets of disease severity and exacerbation risk. The combination of low BEC with high FeNO appeared to indicate a lower risk of exacerbation. However, Pseudomonas aeruginosa colonization and a high neutrophil-to-lymphocyte ratio (NLR ≥ 3.0) were identified as more significant predictors of exacerbation frequency, independent of type 2 biomarker presence.
Conclusions: Our study underscores the distinct roles of type 2 biomarkers, highlighting BEC and FeNO, in bronchiectasis for assessing disease severity and predicting exacerbation risk. It advocates for a multi-biomarker strategy, incorporating these with microbiological and clinical assessments, for comprehensive patient management.
Keywords: Pseudomonas aeruginosa; Blood eosinophil count; Bronchiectasis; Fractional exhaled nitric oxide; Immunoglobulin E; Type 2 biomarkers.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Comment in
-
Type 2 Biomarkers and Bronchiectasis.Lung. 2024 Aug;202(4):365-366. doi: 10.1007/s00408-024-00716-z. Lung. 2024. PMID: 38884648 No abstract available.
References
-
- Polverino E, Goeminne PC, McDonnell MJ et al (2017) European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J 50:1700629 - PubMed
-
- Tiew PY, Jaggi TK, Chan LLY et al (2021) The airway microbiome in COPD, bronchiectasis and bronchiectasis-COPD overlap. Clin Respir J 15:123 - PubMed
-
- Guan WJ, Oscullo G, He MZ et al (2023) Significance and potential role of eosinophils in non-cystic fibrosis bronchiectasis. J Allergy Clin Immunol Pract 11:1089–1099 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
