

Povidone Iodine vs Chlorhexidine Gluconate in Alcohol for Preoperative Skin Antisepsis: A Randomized Clinical Trial
- PMID: 38884982
- PMCID: PMC11184497
- DOI: 10.1001/jama.2024.8531
Povidone Iodine vs Chlorhexidine Gluconate in Alcohol for Preoperative Skin Antisepsis: A Randomized Clinical Trial
Abstract
Importance: Preoperative skin antisepsis is an established procedure to prevent surgical site infections (SSIs). The choice of antiseptic agent, povidone iodine or chlorhexidine gluconate, remains debated.
Objective: To determine whether povidone iodine in alcohol is noninferior to chlorhexidine gluconate in alcohol to prevent SSIs after cardiac or abdominal surgery.
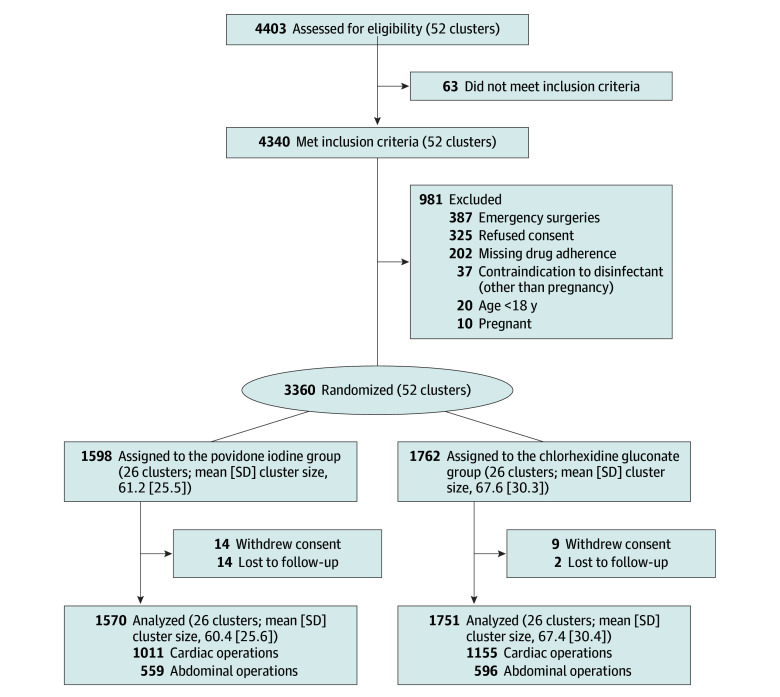
Design, setting, and participants: Multicenter, cluster-randomized, investigator-masked, crossover, noninferiority trial; 4403 patients undergoing cardiac or abdominal surgery in 3 tertiary care hospitals in Switzerland between September 2018 and March 2020 were assessed and 3360 patients were enrolled (cardiac, n = 2187 [65%]; abdominal, n = 1173 [35%]). The last follow-up was on July 1, 2020.
Interventions: Over 18 consecutive months, study sites were randomly assigned each month to either use povidone iodine or chlorhexidine gluconate, each formulated in alcohol. Disinfectants and skin application processes were standardized and followed published protocols.
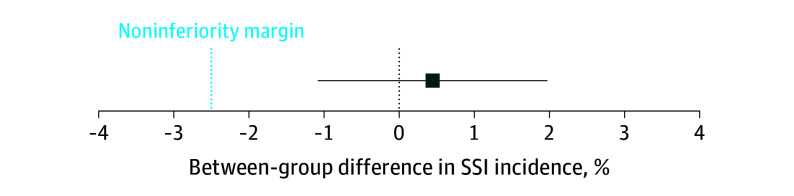
Main outcomes and measures: Primary outcome was SSI within 30 days after abdominal surgery and within 1 year after cardiac surgery, using definitions from the US Centers for Disease Control and Prevention's National Healthcare Safety Network. A noninferiority margin of 2.5% was used. Secondary outcomes included SSIs stratified by depth of infection and type of surgery.
Results: A total of 1598 patients (26 cluster periods) were randomly assigned to receive povidone iodine vs 1762 patients (26 cluster periods) to chlorhexidine gluconate. Mean (SD) age of patients was 65.0 years (39.0-79.0) in the povidone iodine group and 65.0 years (41.0-78.0) in the chlorhexidine gluconate group. Patients were 32.7% and 33.9% female in the povidone iodine and chlorhexidine gluconate groups, respectively. SSIs were identified in 80 patients (5.1%) in the povidone iodine group vs 97 (5.5%) in the chlorhexidine gluconate group, a difference of 0.4% (95% CI, -1.1% to 2.0%) with the lower limit of the CI not exceeding the predefined noninferiority margin of -2.5%; results were similar when corrected for clustering. The unadjusted relative risk for povidone iodine vs chlorhexidine gluconate was 0.92 (95% CI, 0.69-1.23). Nonsignificant differences were observed following stratification by type of surgical procedure. In cardiac surgery, SSIs were present in 4.2% of patients with povidone iodine vs 3.3% with chlorhexidine gluconate (relative risk, 1.26 [95% CI, 0.82-1.94]); in abdominal surgery, SSIs were present in 6.8% with povidone iodine vs 9.9% with chlorhexidine gluconate (relative risk, 0.69 [95% CI, 0.46-1.02]).
Conclusions and relevance: Povidone iodine in alcohol as preoperative skin antisepsis was noninferior to chlorhexidine gluconate in alcohol in preventing SSIs after cardiac or abdominal surgery.
Trial registration: ClinicalTrials.gov Identifier: NCT03685604.
Conflict of interest statement
Figures
Comment in
-
Skin Antisepsis to Prevent Surgical Site Infections: Implications for Global Surgery.JAMA. 2024 Aug 20;332(7):550. doi: 10.1001/jama.2024.9622. JAMA. 2024. PMID: 38884966 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
