

Association of Residential Greenness Exposure with Depression Incidence in Adults 50 Years of Age and Older: Findings from the Cohort Study on Global AGEing and Adult Health (SAGE) in China
- PMID: 38885140
- PMCID: PMC11218708
- DOI: 10.1289/EHP13947
Association of Residential Greenness Exposure with Depression Incidence in Adults 50 Years of Age and Older: Findings from the Cohort Study on Global AGEing and Adult Health (SAGE) in China
Abstract
Background: Depression is a social and public health problem of great concern globally. Identifying and managing the factors influencing depression are crucial for preventing and decreasing the burden of depression.
Objectives: Our objectives are to explore the association between residential greenness and the incidence of depression in an older Chinese population and to calculate the disease burden of depression prevented by greenness exposure.
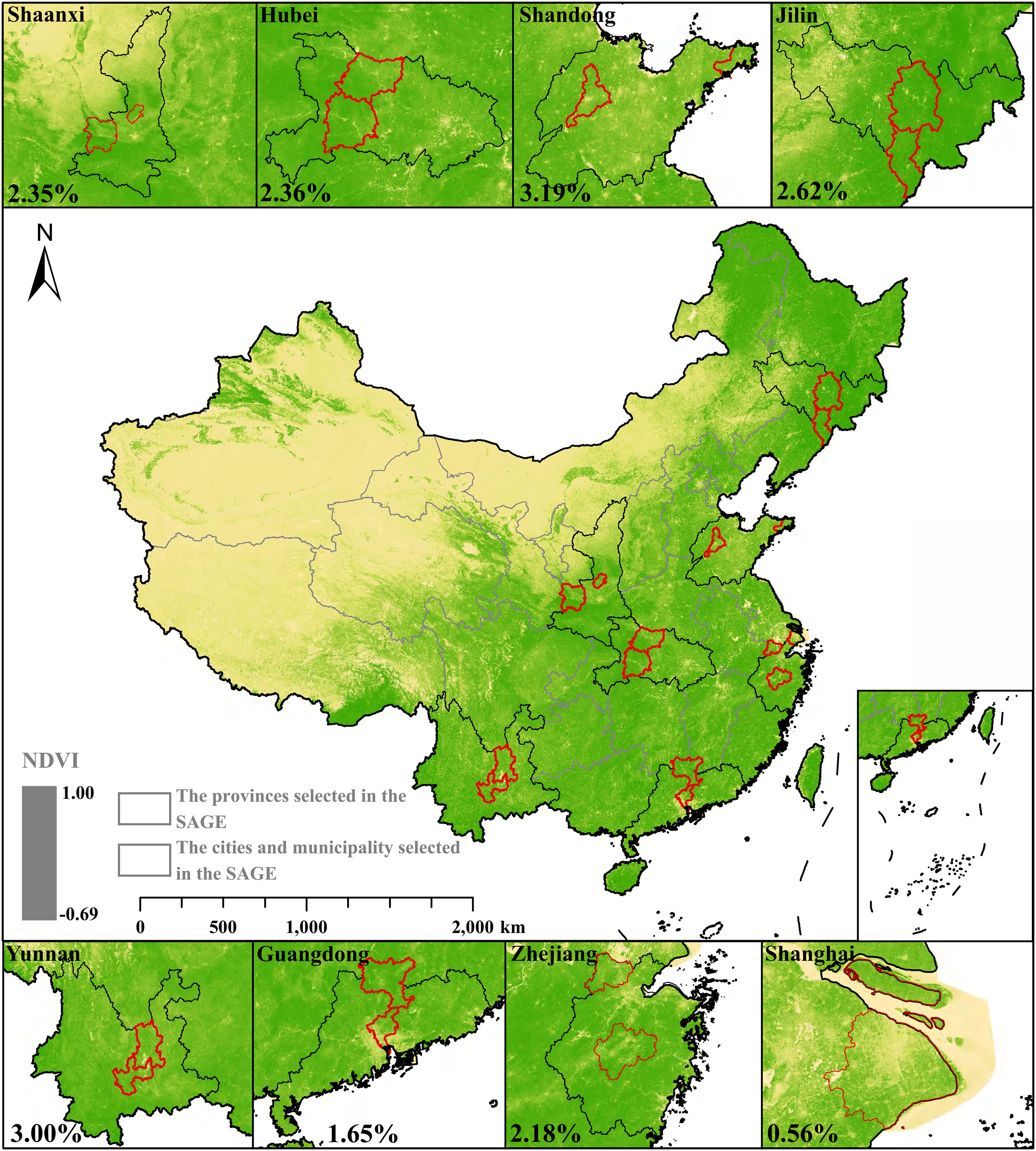
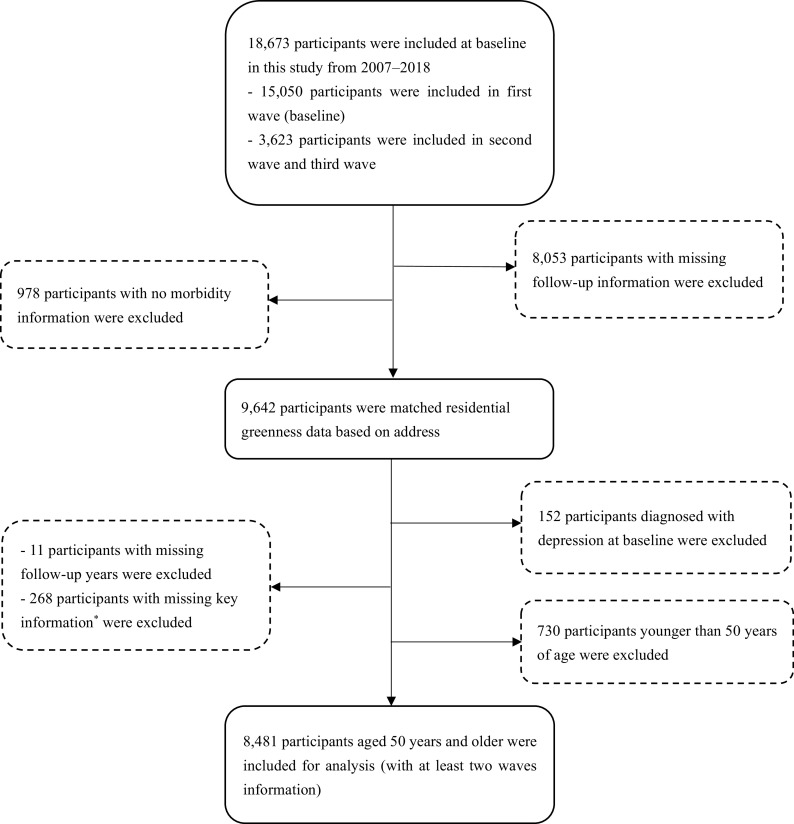
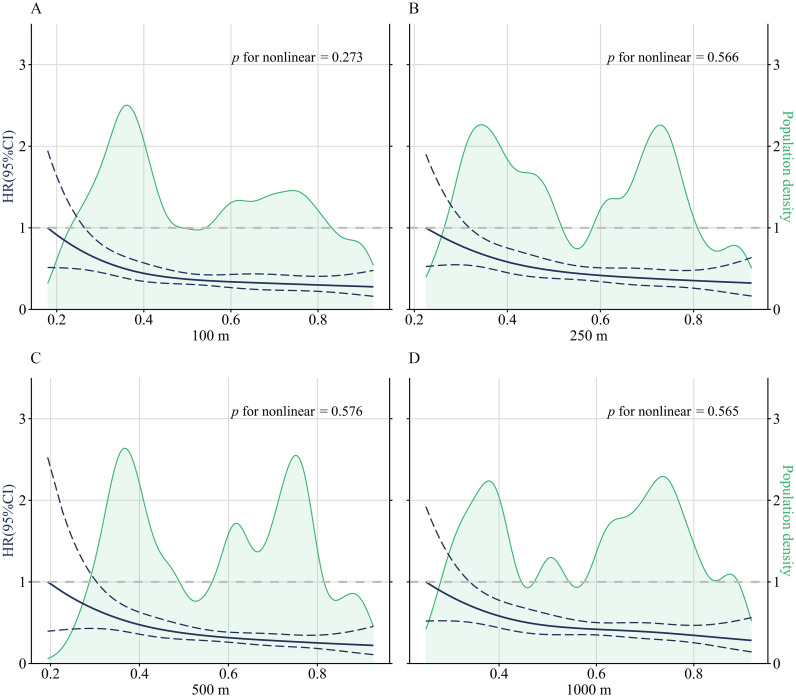
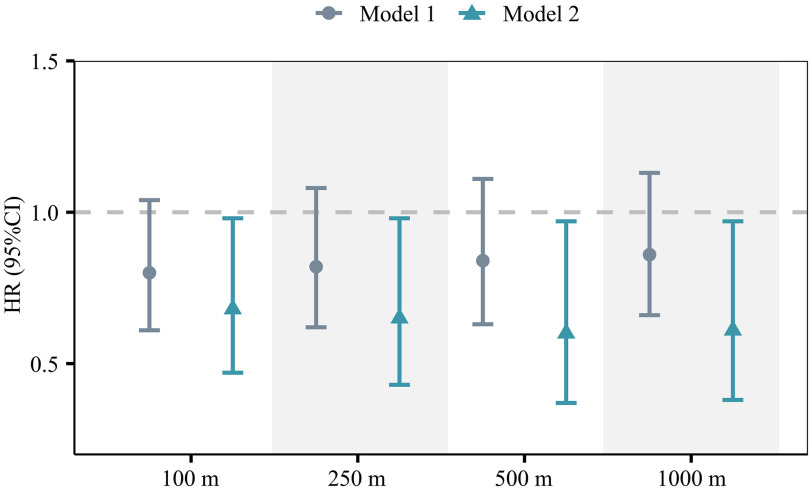
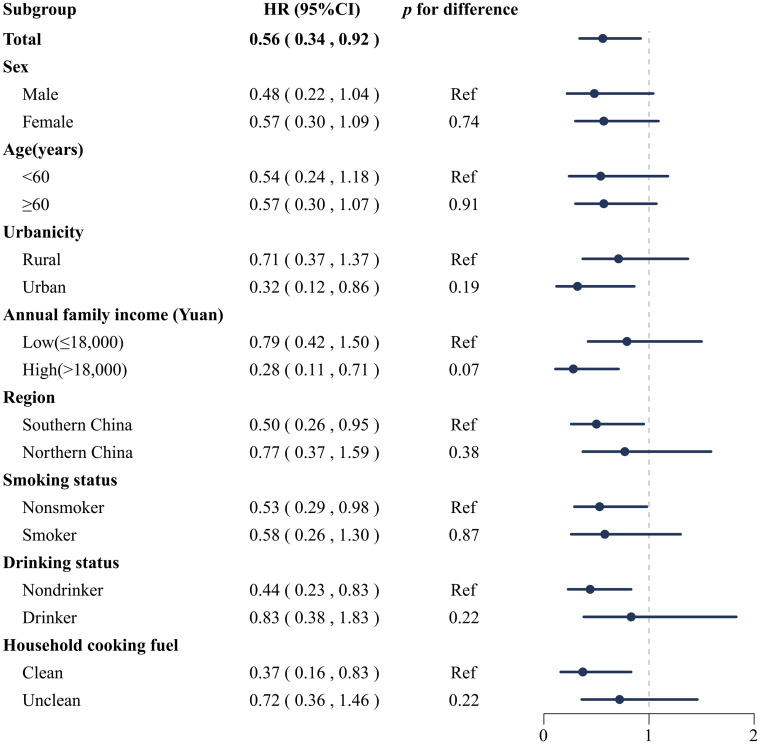
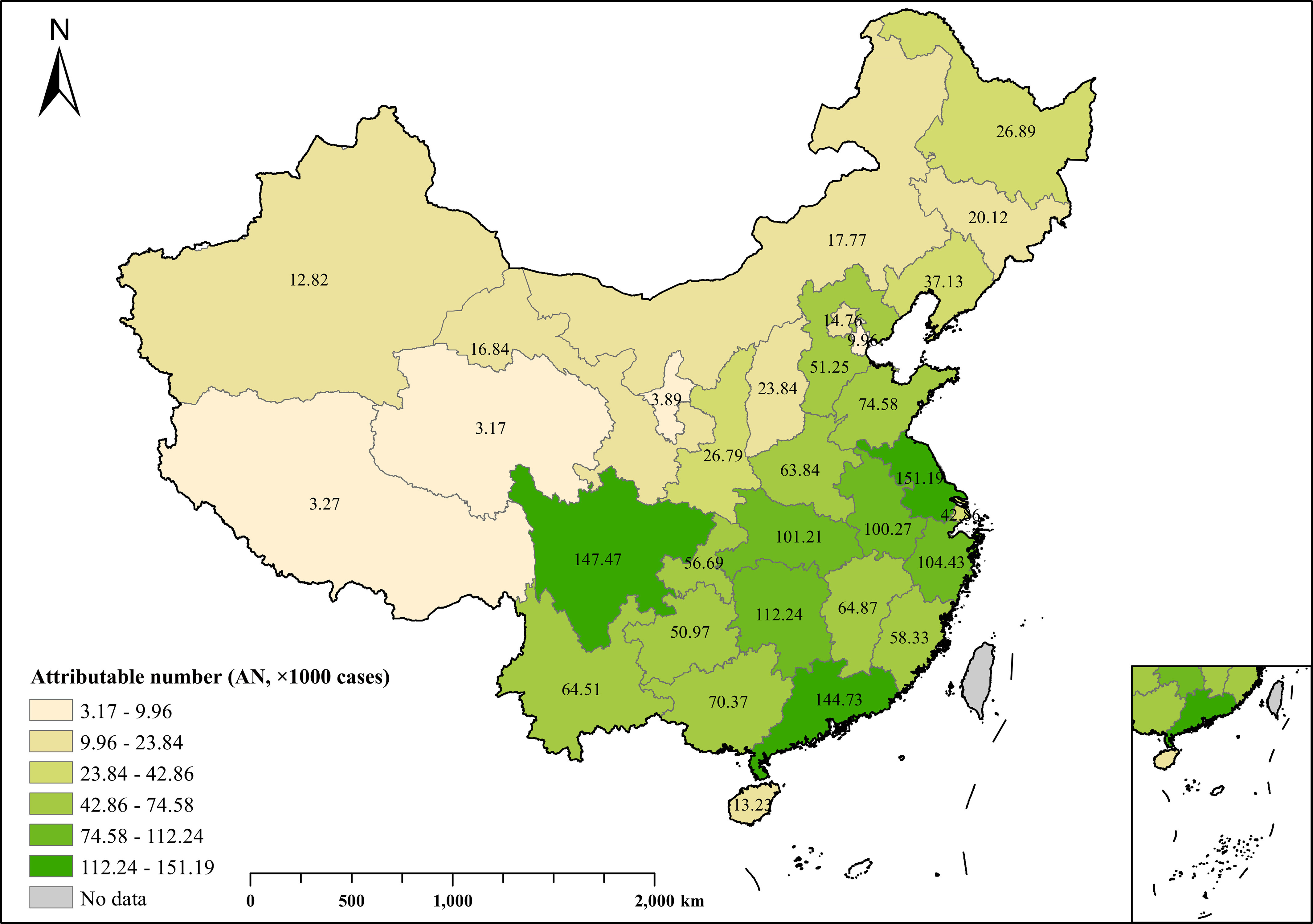
Methods: This study was the Chinese part of the World Health Organization Study on Global AGEing and Adult Health (WHO SAGE). We collected the data of 8,481 residents years of age in China for the period 2007-2018. Average follow-up duration was 7.00 () years. Each participant was matched to the yearly maximum normalized difference vegetation index (NDVI) at their residential address. Incidence of depression was assessed using the Composite International Diagnostic Interview (CIDI), self-reports of depression, and/or taking depression medication. Association between greenness and depression was examined using the time-dependent Cox regression model with stratified analysis by sex, age, urbanicity, annual family income, region, smoking, drinking, and household cooking fuels. Furthermore, the prevented fraction (PF) and attributable number (AN) of depression prevented by exposure to greenness were estimated.
Results: Residential greenness was negatively associated with depression. Each interquartile range (IQR) increase in NDVI buffer was associated with a 40% decrease [; 95% confidence interval (CI): 0.37, 0.97] in the risk of depression incidence among the total participants. Subgroup analyses showed negative associations in urban residents (; 95% CI: 0.12, 0.86) vs. rural residents, in high-income residents (; 95% CI: 0.11, 0.71) vs. low-income residents, and in southern China (; 95% CI: 0.26, 0.95) vs. northern China. Over 8.0% (; 95% CI: 1.38%, 15.40%) and 1,955,199 (95% CI: 310,492; 3,464,909) new cases of depression may be avoided by increasing greenness exposures annually across China.
Discussion: The findings suggest protective effects of residential greenness exposure on depression incidence in the older population, particularly among urban residents, high-income residents, and participants living in southern China. The construction of residential greenness should be included in community planning. https://doi.org/10.1289/EHP13947.
Figures
Similar articles
-
Association of residential greenness exposures on disability: Findings from the cohort study on global AGEing and Adult Health (SAGE) in China.Environ Res. 2025 Jan 1;264(Pt 1):120358. doi: 10.1016/j.envres.2024.120358. Epub 2024 Nov 13. Environ Res. 2025. PMID: 39542158
-
Association between residential greenness and depression symptoms in Chinese community-dwelling older adults.Environ Res. 2024 Feb 15;243:117869. doi: 10.1016/j.envres.2023.117869. Epub 2023 Dec 7. Environ Res. 2024. PMID: 38070849
-
Association of residential greenness and incident depression: Investigating the mediation and interaction effects of particulate matter.Sci Total Environ. 2022 Mar 10;811:152372. doi: 10.1016/j.scitotenv.2021.152372. Epub 2021 Dec 14. Sci Total Environ. 2022. PMID: 34914979
-
Residential greenness and risks of depression: Longitudinal associations with different greenness indicators and spatial scales in a Finnish population cohort.Health Place. 2022 Mar;74:102760. doi: 10.1016/j.healthplace.2022.102760. Epub 2022 Feb 5. Health Place. 2022. PMID: 35134742 Review.
-
Surrounding Residential Greenness and Health: Associations With Abdominal Obesity and Dyslipidemia. A Meta-Analysis of Cross-Sectional Studies.Public Health Rev. 2025 Feb 18;46:1608163. doi: 10.3389/phrs.2025.1608163. eCollection 2025. Public Health Rev. 2025. PMID: 40047002 Free PMC article.
Cited by
-
The non-linear relationship between atherogenic index of plasma and stroke: a study among middle-aged and elderly Chinese adults with depression.Lipids Health Dis. 2025 Jul 1;24(1):224. doi: 10.1186/s12944-025-02641-3. Lipids Health Dis. 2025. PMID: 40598527 Free PMC article.
-
Association between social media use and depressive symptoms in middle-aged and older Chinese adults.Transl Psychiatry. 2024 Oct 11;14(1):430. doi: 10.1038/s41398-024-03142-0. Transl Psychiatry. 2024. PMID: 39394184 Free PMC article.
-
Greenspace proximity in relation to sleep health among a racially and ethnically diverse cohort of US women.Environ Res. 2025 Aug 15;279(Pt 1):121698. doi: 10.1016/j.envres.2025.121698. Epub 2025 Apr 25. Environ Res. 2025. PMID: 40288743
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
