

Lateral episiotomy or no episiotomy in vacuum assisted delivery in nulliparous women (EVA): multicentre, open label, randomised controlled trial
- PMID: 38886011
- PMCID: PMC11307825
- DOI: 10.1136/bmj-2023-079014
Lateral episiotomy or no episiotomy in vacuum assisted delivery in nulliparous women (EVA): multicentre, open label, randomised controlled trial
Abstract
Objective: To assess the effect of lateral episiotomy, compared with no episiotomy, on obstetric anal sphincter injury in nulliparous women requiring vacuum extraction.
Design: A multicentre, open label, randomised controlled trial.
Setting: Eight hospitals in Sweden, 2017-23.
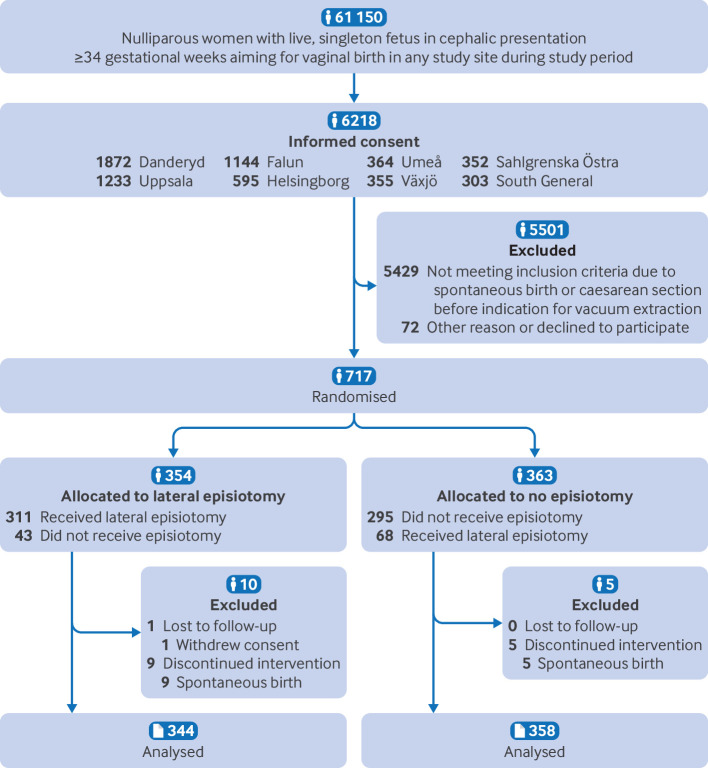
Participants: 717 nulliparous women with a single live fetus of 34 gestational weeks or more, requiring vacuum extraction were randomly assigned (1:1) to lateral episiotomy or no episiotomy using sealed opaque envelopes. Randomisation was stratified by study site.
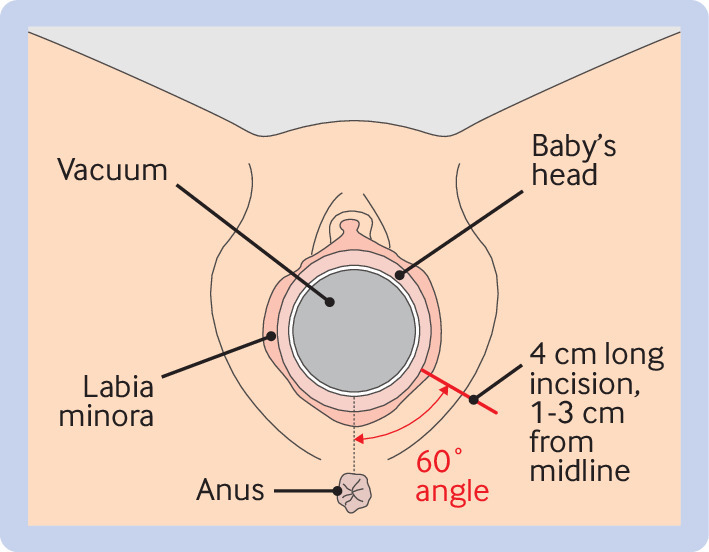
Intervention: A standardised lateral episiotomy was performed during the vacuum extraction, at crowning of the fetal head, starting 1-3 cm from the posterior fourchette, at a 60° (45-80°) angle from the midline, and 4 cm (3-5 cm) long. The comparison was no episiotomy unless considered indispensable.
Main outcome measures: The primary outcome of the episiotomy in vacuum assisted delivery (EVA) trial was obstetric anal sphincter injury, clinically diagnosed by combined visual inspection and digital rectal and vaginal examination. The primary analysis used a modified intention-to-treat population that included all consenting women with attempted or successful vacuum extraction. As a result of an interim analysis at significance level P<0.01, the primary endpoint was tested at 4% significance level with accompanying 96% confidence interval (CI).
Results: From 1 July 2017 to 15 February 2023, 717 women were randomly assigned: 354 (49%) to lateral episiotomy and 363 (51%) to no episiotomy. Before vacuum extraction attempt, one woman withdrew consent and 14 had a spontaneous birth, leaving 702 for the primary analysis. In the intervention group, 21 (6%) of 344 women sustained obstetric anal sphincter injury, compared with 47 (13%) of 358 women in the comparison group (P=0.002). The risk difference was -7.0% (96% CI -11.7% to -2.5%). The risk ratio adjusted for site was 0.47 (96% CI 0.23 to 0.97) and unadjusted risk ratio was 0.46 (0.28 to 0.78). No significant differences were noted between groups in postpartum pain, blood loss, neonatal outcomes, or total adverse events, but the intervention group had more wound infections and dehiscence.
Conclusions: Lateral episiotomy can be recommended for nulliparous women requiring vacuum extraction to significantly reduce the risk of obstetric anal sphincter injury.
Trial registration: ClinicalTrials.gov NCT02643108.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: funding from the Swedish Research Council (2016-00526), the Stockholm Region (FoUI-960261/2021), and the Uppsala-Örebro Research Council (RFR-939428); no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; and no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Swedish Agency for Health Technology Assessment and Assessment of Social Services. SBU Systematic Review Summaries. Anal sphincter injuries: a systematic review and assessment of medical, social and ethical aspects. Stockholm: Swedish Council on Health Technology Assessment (SBU). 2016.
-
- Blondel B, Alexander S, Bjarnadóttir RI, et al. Euro-Peristat Scientific Committee . Variations in rates of severe perineal tears and episiotomies in 20 European countries: a study based on routine national data in Euro-Peristat Project. Acta Obstet Gynecol Scand 2016;95:746-54. 10.1111/aogs.12894. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials