

Differential cortical layer engagement during seizure initiation and spread in humans
- PMID: 38886376
- PMCID: PMC11183216
- DOI: 10.1038/s41467-024-48746-8
Differential cortical layer engagement during seizure initiation and spread in humans
Abstract
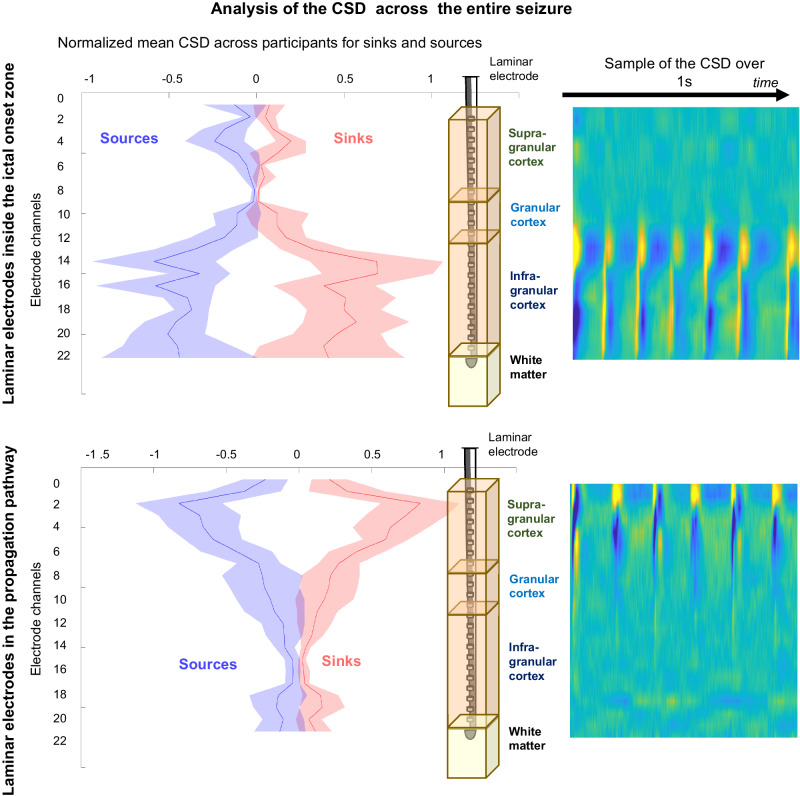
Despite decades of research, we still do not understand how spontaneous human seizures start and spread - especially at the level of neuronal microcircuits. In this study, we used laminar arrays of micro-electrodes to simultaneously record the local field potentials and multi-unit neural activities across the six layers of the neocortex during focal seizures in humans. We found that, within the ictal onset zone, the discharges generated during a seizure consisted of current sinks and sources only within the infra-granular and granular layers. Outside of the seizure onset zone, ictal discharges reflected current flow in the supra-granular layers. Interestingly, these patterns of current flow evolved during the course of the seizure - especially outside the seizure onset zone where superficial sinks and sources extended into the deeper layers. Based on these observations, a framework describing cortical-cortical dynamics of seizures is proposed with implications for seizure localization, surgical targeting, and neuromodulation techniques to block the generation and propagation of seizures.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Rugg-Gunn F, Miserocchi A, McEvoy A. Epilepsy surgery. Pr. Neurol. 2020;20:4–14. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
