

Fitting in? Physician practice style after forced relocation
- PMID: 38886564
- PMCID: PMC11249821
- DOI: 10.1111/1475-6773.14340
Fitting in? Physician practice style after forced relocation
Abstract
Objective: This study aims to examine how variation in physicians' treatment decisions for newborn deliveries responds to changes in the hospital-level norms for obstetric clinical decision-making.
Data sources: All hospital-based births in Florida from 2003 through 2017.
Study design: Difference-in-differences approach is adopted that leverages obstetric unit closures as the source of identifying variation to exogenously shift obstetricians to a new, nearby hospital with different propensities to approach newborn deliveries less intensively.
Data extraction: Births attributed to physicians continuously observed 2 years before the closure event and 2 years after the closure event (treatment group physicians) or for identical time periods around a randomly assigned placebo closure date (control group physicians).
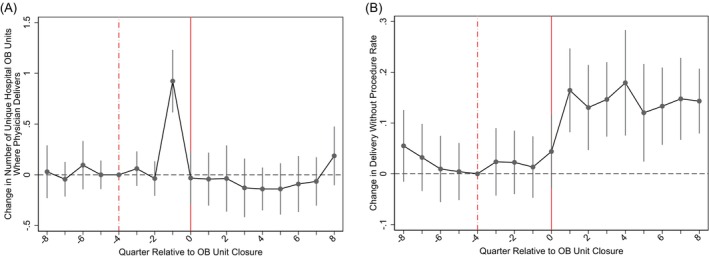
Principal findings: All of the physicians meeting our inclusion criteria shifted their births to a new hospital less than 20 miles from the hospital shuttering its obstetric unit. The new hospitals approached newborn births more conservatively, and treatment group physicians sharply became less aggressive in their newborn birth clinical management (e.g., use of C-section). The immediate 11-percentage point (33%) increase in delivering newborns without any procedure behavior change is statistically significant (p value <0.01) and persistent after the closure event; however, the physicians' payer and patient mix are unchanged.
Conclusions: Obstetric physician behavior change appears highly malleable and sensitive to the practice patterns of other physicians delivering newborns at the same hospital. Incentives and policies that encourage more appropriate clinical care norms hospital-wide could sharply improve physician treatment decisions, with benefits for maternal and infant outcomes.
Keywords: newborn deliveries; obstetric unit closures; obstetrics; physician practice patterns.
© 2024 Health Research and Educational Trust.
Figures
Similar articles
-
The Perinatal Committee report: Review of the progress of obstetric healthcare in Japan.J Obstet Gynaecol Res. 2025 Jul;51(7):e16354. doi: 10.1111/jog.16354. J Obstet Gynaecol Res. 2025. PMID: 40690975 Free PMC article. Review.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Maternal and neonatal outcomes of elective induction of labor.Evid Rep Technol Assess (Full Rep). 2009 Mar;(176):1-257. Evid Rep Technol Assess (Full Rep). 2009. PMID: 19408970 Free PMC article.
-
Analysis of deliveries using the Robson Classification System in a Brazilian hospital: a cross-sectional observational study.J Obstet Gynaecol. 2025 Dec;45(1):2522867. doi: 10.1080/01443615.2025.2522867. Epub 2025 Jun 25. J Obstet Gynaecol. 2025. PMID: 40560744
-
The effect of waterbirth on neonatal mortality and morbidity: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2015 Oct;13(10):180-231. doi: 10.11124/jbisrir-2015-2105. JBI Database System Rev Implement Rep. 2015. PMID: 26571292
Cited by
-
Analysis of the current situation and influencing factors of nurse change fatigue.Front Public Health. 2025 Apr 9;13:1566534. doi: 10.3389/fpubh.2025.1566534. eCollection 2025. Front Public Health. 2025. PMID: 40270743 Free PMC article.
References
-
- Phelps CE. Information diffusion and best practice adoption. In: Culyer AJ, Newhouse JP, eds. Handbook of Health Economics. Vol 1A. Elsevier Science B.V.; 2000:223‐264.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
