

Peripheral blood mononuclear cell respiratory function is associated with progressive glaucomatous vision loss
- PMID: 38886621
- PMCID: PMC11333286
- DOI: 10.1038/s41591-024-03068-6
Peripheral blood mononuclear cell respiratory function is associated with progressive glaucomatous vision loss
Abstract
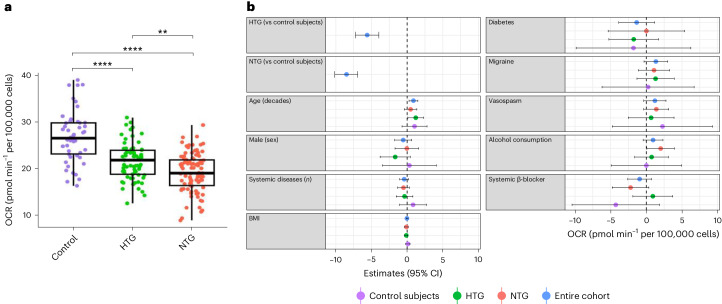
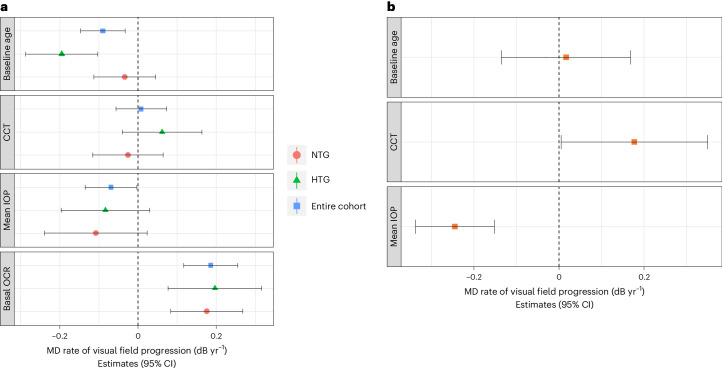
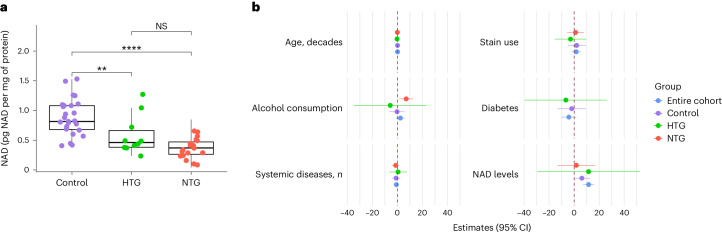
Intraocular pressure (IOP) is currently the only modifiable risk factor for glaucoma and all licensed treatments lower IOP. However, many patients continue to lose vision despite IOP-lowering treatment. Identifying biomarkers for progressive vision loss would have considerable clinical utility. We demonstrate that lower peripheral blood mononuclear cell (PBMC) oxygen consumption rate (OCR) is strongly associated with faster visual field (VF) progression in patients treated by lowering IOP (P < 0.001, 229 eyes of 139 participants), explaining 13% of variance in the rate of progression. In a separate reference cohort of untreated patients with glaucoma (213 eyes of 213 participants), IOP explained 16% of VF progression variance. OCR is lower in patients with glaucoma (n = 168) than in controls (n = 50; P < 0.001) and is lower in patients with low baseline IOP (n = 99) than those with high baseline IOP (n = 69; P < 0.01). PBMC nicotinamide adenine dinucleotide (NAD) levels are lower in patients with glaucoma (n = 29) compared to controls (n = 25; P < 0.001) and strongly associated with OCR (P < 0.001). Our results support PBMC OCR and NAD levels as new biomarkers for progressive glaucoma.
© 2024. The Author(s).
Conflict of interest statement
D.G.-H. received consultation fees from Abbvie, Janssen, Omikron, Roche, Santen and Viatris. G.M. received consultation fees from Alcon and Omikron. G.L. has research funding from Aerie, Abbvie and other remuneration received by Glaukos and Rayner. P.A.W. is an inventor on an awarded US patent held by The Jackson Laboratory for NAM treatment in glaucoma (Treatment and prevention of ocular neurodegenerative disorder, US11389439B2).
Figures
References
-
- Quigley, H. A. Glaucoma. Lancet377, 1367–1377 (2011). - PubMed
-
- Heijl, A., Leske, M. C., Bengtsson, B., Bengtsson, B. & Hussein, M. Measuring visual field progression in the Early Manifest Glaucoma Trial. Acta Ophthalmol. Scand.81, 286–293 (2003). - PubMed
-
- Garway-Heath, D. F. et al. Latanoprost for open-angle glaucoma (UKGTS): a randomised, multicentre, placebo-controlled trial. Lancet385, 1295–1304 (2015). - PubMed
-
- Investigators, A. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am. J. Ophthalmol.130, 429–440 (2000). - PubMed
-
- Heijl, A. et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol.120, 1268–1279 (2002). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
