

Personalized brain circuit scores identify clinically distinct biotypes in depression and anxiety
- PMID: 38886626
- PMCID: PMC11271415
- DOI: 10.1038/s41591-024-03057-9
Personalized brain circuit scores identify clinically distinct biotypes in depression and anxiety
Abstract
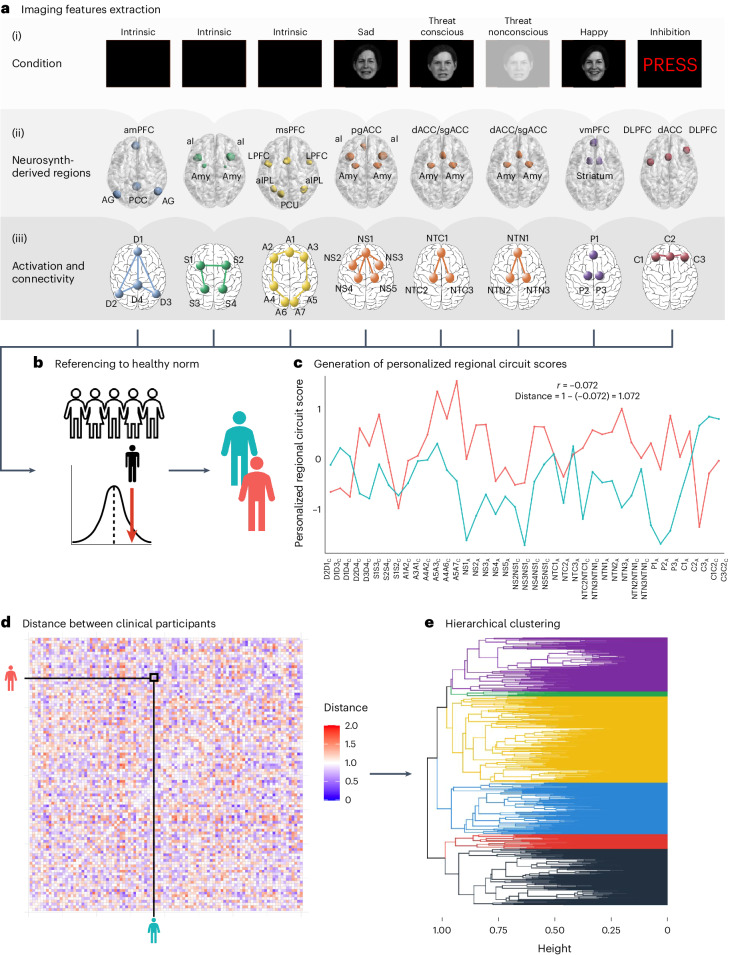
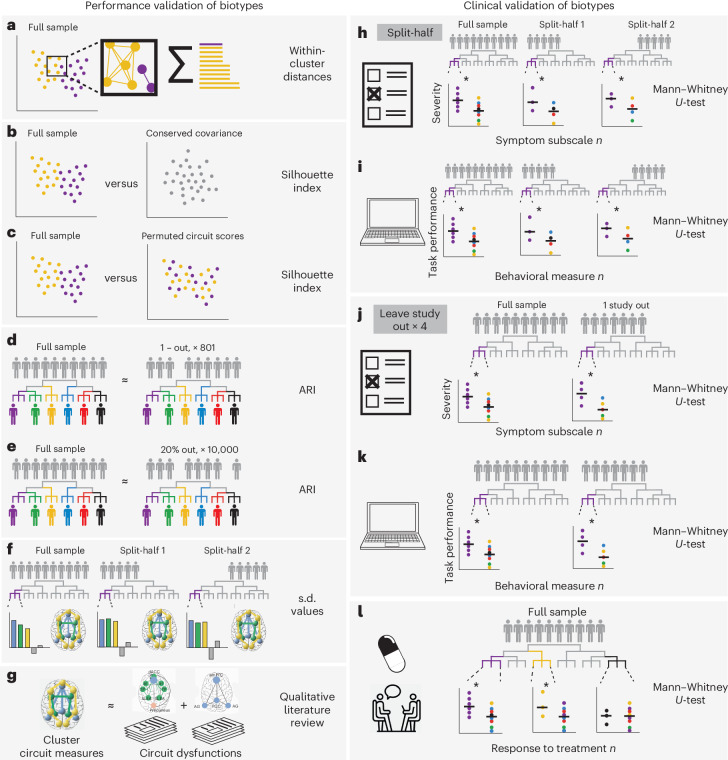
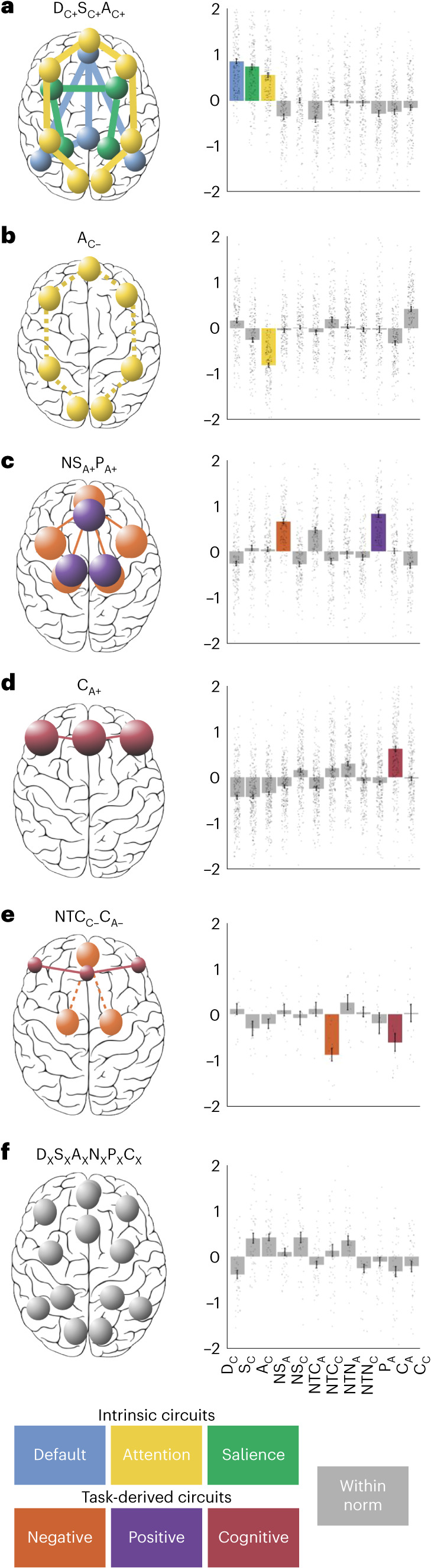
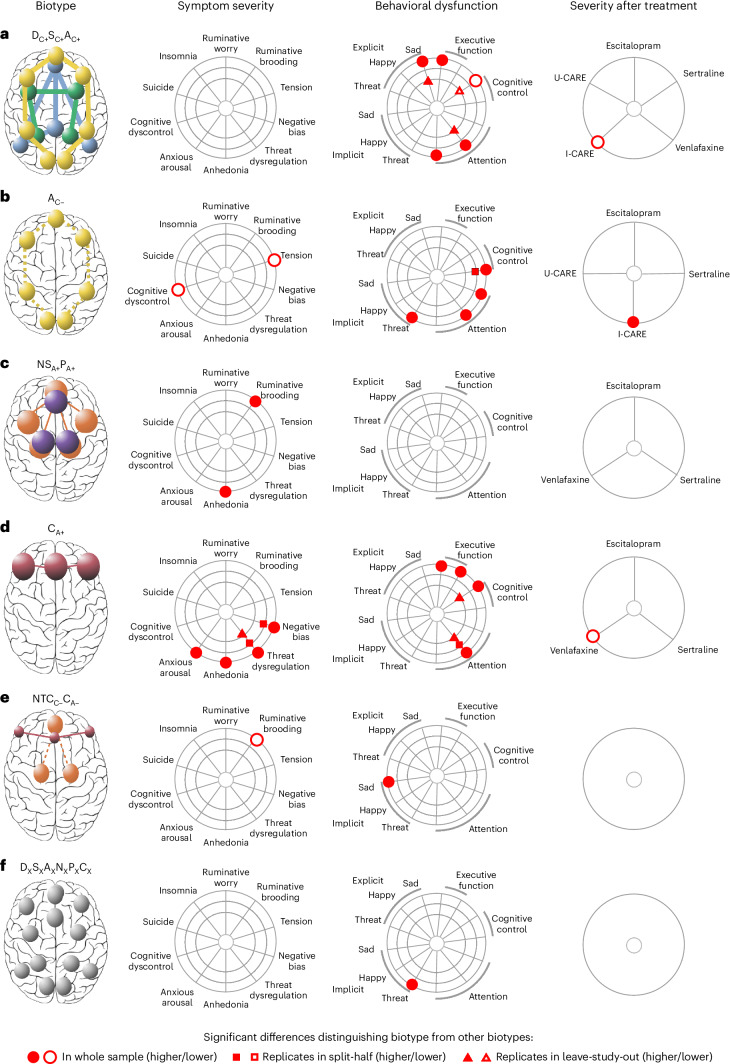
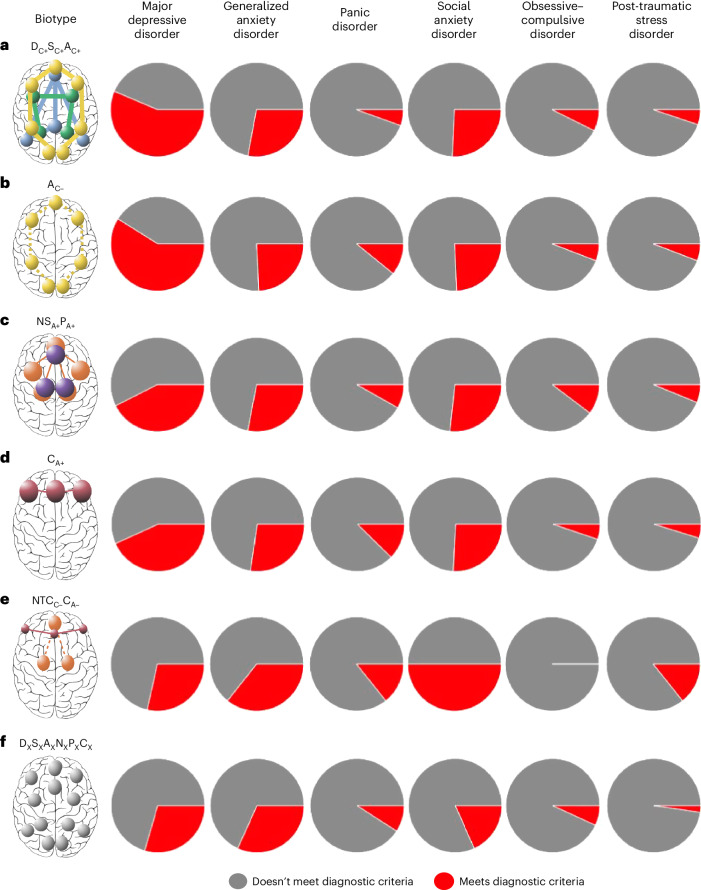
There is an urgent need to derive quantitative measures based on coherent neurobiological dysfunctions or 'biotypes' to enable stratification of patients with depression and anxiety. We used task-free and task-evoked data from a standardized functional magnetic resonance imaging protocol conducted across multiple studies in patients with depression and anxiety when treatment free (n = 801) and after randomization to pharmacotherapy or behavioral therapy (n = 250). From these patients, we derived personalized and interpretable scores of brain circuit dysfunction grounded in a theoretical taxonomy. Participants were subdivided into six biotypes defined by distinct profiles of intrinsic task-free functional connectivity within the default mode, salience and frontoparietal attention circuits, and of activation and connectivity within frontal and subcortical regions elicited by emotional and cognitive tasks. The six biotypes showed consistency with our theoretical taxonomy and were distinguished by symptoms, behavioral performance on general and emotional cognitive computerized tests, and response to pharmacotherapy as well as behavioral therapy. Our results provide a new, theory-driven, clinically validated and interpretable quantitative method to parse the biological heterogeneity of depression and anxiety. Thus, they represent a promising approach to advance precision clinical care in psychiatry.
© 2024. The Author(s).
Conflict of interest statement
L.M.W. declares US patent application nos. 10/034,645 and 15/820,338: ‘Systems and methods for detecting complex networks in MRI data’. In the past 3 years L.M.H. participated on a Roche Advisory Board. L.T. has been employed by Ceribell Inc. since 30 October 2023. The remaining authors declare no competing interests.
Figures
References
-
- Friedrich, M. J. Depression is the leading cause of disability around the world. JAMA317, 1517 (2017). - PubMed
MeSH terms
Grants and funding
- U01MH136062/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- U01MH109985/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- UH2HL132368/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- U01MH109985/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- U01 MH109985/MH/NIMH NIH HHS/United States
- UH2HL132368/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- U01 MH136062/MH/NIMH NIH HHS/United States
- UH2 HL132368/HL/NHLBI NIH HHS/United States
- R01MH101496/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- R01 MH101496/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
