

Predictors of futile recanalization after endovascular treatment of acute ischemic stroke
- PMID: 38886670
- PMCID: PMC11181662
- DOI: 10.1186/s12883-024-03719-8
Predictors of futile recanalization after endovascular treatment of acute ischemic stroke
Abstract
Objective: Endovascular therapy (EVT) is the most successful treatment for patients with acute ischemic stroke (AIS) due to large vessel occlusion (LVO) in the anterior circulation. However, futile recanalization (FR) seriously affects the prognosis of these patients. The aim of this study was to investigate predictors of FR after EVT in patients with AIS.
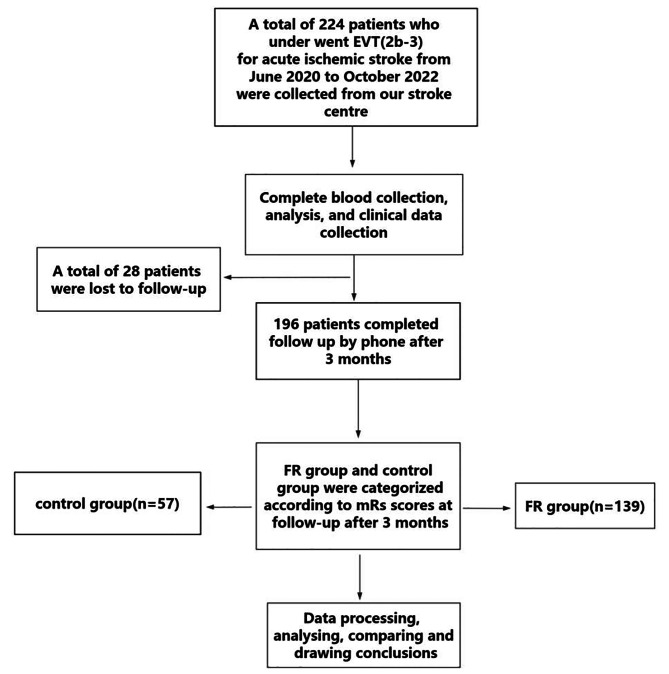
Method: Patients diagnosed with AIS due to anterior circulation LVO and receiving EVT between June 2020 and October 2022 were prospectively enrolled. FR after EVT was defined as a poor 90-day prognosis (modified Rankin Scale [mRS] score ≥ 3) despite achieving successful reperfusion (modified Thrombolysis in Cerebral Infarction [mTICI] classification of 2b-3). All included patients were categorized into control group (mRS score < 3) and FR group (mRS score ≥ 3). Demographic characteristics, comorbidities (hypertension, diabetes, atrial fibrillation, smoking, etc.), stroke-specific data (NIHSS score, ASPECT score and site of occlusion), procedure data (treatment type [direct thrombectomy vs. bridging thrombectomy], degree of vascular recanalization [mTICI], procedure duration time and onset-recanalization time), laboratory indicators (lymphocytes count, neutrophils count, monocytes count, C-reactive protein, neutrophil-to-lymphocyte ratio [NLR], monocyte-to-high-density lipoprotein ratio [MHR], lymphocyte-to-monocyte ratio [LMR], lymphocyte-to-C-reactive protein ratio [LCR], lymphocyte-to-high-density lipoprotein ratio[LHR], total cholesterol and triglycerides.) were compared between the two groups. Multivariate logistic regression analysis was performed to explore independent predictors of FR after EVT.
Results: A total of 196 patients were included in this study, among which 57 patients were included in the control group and 139 patients were included in the FR group. Age, proportion of patients with hypertension and diabetes mellitus, median NIHSS score, CRP level, procedure duration time, neutrophil count and NLR were higher in the FR group than in the control group. Lymphocyte count, LMR, and LCR were lower in the FR group than in the control group. There were no significant differences in platelet count, monocytes count, total cholesterol, triglycerides, HDL, LDL, gender, smoking, atrial fibrillation, percentage of occluded sites, onset-recanalization time, ASPECT score and type of treatment between the two groups. Multivariate logistic regression analysis demonstrated that NLR was independently associated with FR after EVT (OR = 1.37, 95%CI = 1.005-1.86, P = 0.046).
Conclusion: This study demonstrated that high NLR was associated with a risk of FR in patients with AIS due to anterior circulation LVO. These findings may help clinicians determine which patients with AIS are at higher risk of FR after EVT. Our study can provide a theoretical basis for interventions in the aforementioned population.
Keywords: Acute ischemic stroke; Endovascular treatment; Futile recanalization; Neutrophil-to-lymphocyte ratio.
© 2024. The Author(s).
Conflict of interest statement
None of the authors have identified a conflict of interest.
Similar articles
-
Futile recanalization after endovascular treatment in acute ischemic stroke with large ischemic core.BMC Neurol. 2024 Oct 16;24(1):395. doi: 10.1186/s12883-024-03912-9. BMC Neurol. 2024. PMID: 39415132 Free PMC article.
-
[Influencing factors of futile recanalization after endovascular therapy in acute ischemic stroke patients with large vessel occlusions].Zhonghua Yi Xue Za Zhi. 2023 Aug 8;103(29):2218-2224. doi: 10.3760/cma.j.cn112137-20230218-00231. Zhonghua Yi Xue Za Zhi. 2023. PMID: 37544757 Chinese.
-
Predictors of futile recanalization in ischemic stroke patients with low baseline NIHSS.Int J Stroke. 2024 Dec;19(10):1102-1112. doi: 10.1177/17474930241264737. Epub 2024 Nov 19. Int J Stroke. 2024. PMID: 38888031 Free PMC article.
-
Endovascular thrombectomy for DAWN- and DEFUSE-3 ineligible acute ischemic stroke patients: a systematic review and meta-analysis.J Neurol. 2024 May;271(5):2230-2237. doi: 10.1007/s00415-024-12198-3. Epub 2024 Feb 3. J Neurol. 2024. PMID: 38308162
-
Comprehensive Meta-Analysis of Futile Recanalization in Acute Ischemic Stroke Patients Undergoing Endovascular Thrombectomy: Prevalence, Factors, and Clinical Outcomes.Life (Basel). 2023 Sep 26;13(10):1965. doi: 10.3390/life13101965. Life (Basel). 2023. PMID: 37895347 Free PMC article. Review.
Cited by
-
Association between hyperglycemia and unfavorable outcome in patients with successful thrombectomy for acute ischemic stroke: a single-center study.BMC Neurol. 2025 Aug 13;25(1):333. doi: 10.1186/s12883-025-04357-4. BMC Neurol. 2025. PMID: 40804609 Free PMC article.
-
Systemic Comorbidities as Modifiers of Outcome After Endovascular Thrombectomy for Acute Ischemic Stroke.Curr Neurol Neurosci Rep. 2025 May 30;25(1):38. doi: 10.1007/s11910-025-01427-5. Curr Neurol Neurosci Rep. 2025. PMID: 40442497 Review.
-
Involvement of Subinsular Territory Stroke as Predictor of Outcome after Successful Endovascular Recanalization of Left Middle Cerebral Artery Occlusion.Brain Sci. 2024 Aug 30;14(9):885. doi: 10.3390/brainsci14090885. Brain Sci. 2024. PMID: 39335381 Free PMC article.
-
Age-Specific Differences in Inflammatory Biomarkers and Their Impact on Futile Recanalization After Mechanical Thrombectomy: An Inverse Probability Weighting Analysis.Eur J Neurol. 2025 May;32(5):e70182. doi: 10.1111/ene.70182. Eur J Neurol. 2025. PMID: 40353608 Free PMC article.
References
-
- Liu L, Chen W, Zhou H, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of ischaemic cerebrovascular diseases. Stroke Vasc Neurol. 2020;5:159–76. doi: 10.1136/svn-2020-000378. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
