

Association between emergency department disposition and mortality in patients with COVID-19 acute respiratory distress syndrome
- PMID: 38887225
- PMCID: PMC11180691
- DOI: 10.1002/emp2.13192
Association between emergency department disposition and mortality in patients with COVID-19 acute respiratory distress syndrome
Abstract
Objectives: Patients hospitalized for COVID-19 frequently develop hypoxemia and acute respiratory distress syndrome (ARDS) after admission. In non-COVID-19 ARDS studies, admission to hospital wards with subsequent transfer to intensive care unit (ICU) is associated with worse outcomes. We hypothesized that initial admission to the ward may affect outcomes in patient with COVID-19 ARDS.
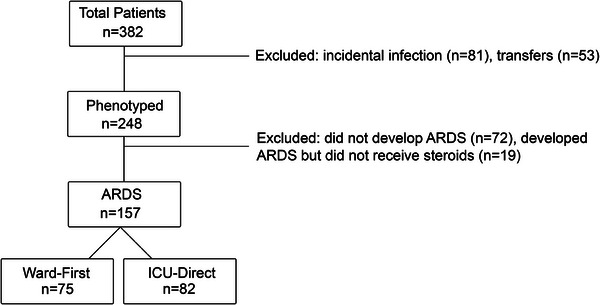
Methods: This was a retrospective study of consecutive adults admitted for COVID-19 ARDS between March 2020 and March 2021 at Stanford Health Care. Mortality scores at hospital admission (Coronavirus Clinical Characterization Consortium Mortality Score [4C score]) and ICU admission (Simplified Acute Physiology Score III [SAPS-III]) were calculated, as well as ROX index for patients on high flow nasal oxygen. Patients were classified by emergency department (ED) disposition (ward-first vs. ICU-direct), and 28- and 60-day mortality and highest level of respiratory support within 1 day of ICU admission were compared. A second cohort (April 2021‒July 2022, n = 129) was phenotyped to validate mortality outcome.
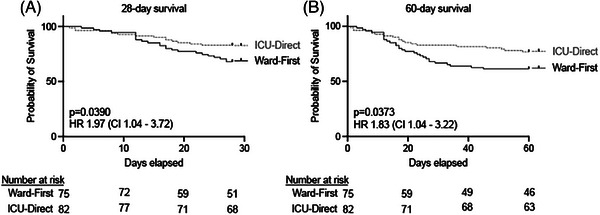
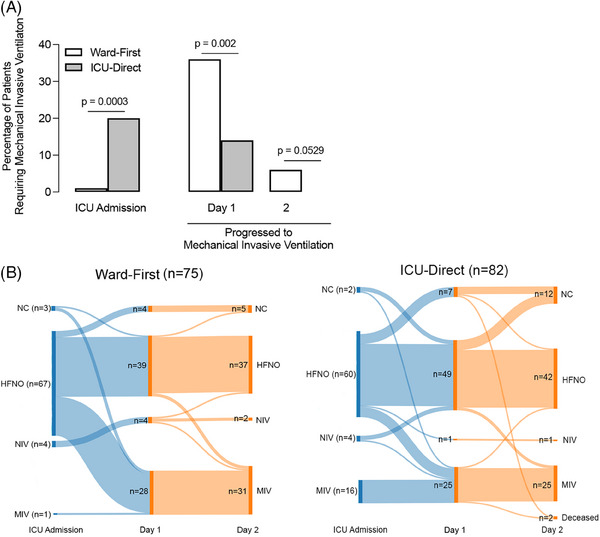
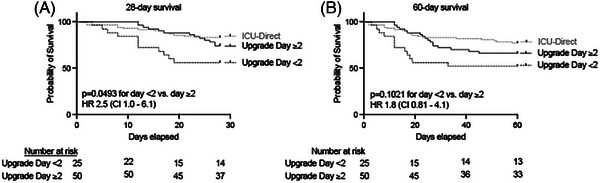
Results: A total of 157 patients were included, 48% of whom were first admitted to the ward (n = 75). Ward-first patients had more comorbidities, including lung disease. Ward-first patients had lower 4C and similar SAPS-III score, yet increased mortality at 28 days (32% vs. 17%, hazard ratio [HR] 2.0, 95% confidence interval [95% CI] 1.0‒3.7, p = 0.039) and 60 days (39% vs. 23%, HR 1.83, 95% CI 1.04‒3.22, p = 0.037) compared to ICU-direct patients. More ward-first patients escalated to mechanical ventilation on day 1 of ICU admission (36% vs. 14%, p = 0.002) despite similar ROX index. Ward-first patients who upgraded to ICU within 48 h of ED presentation had the highest mortality. Mortality findings were replicated in a sensitivity analysis.
Conclusion: Despite similar baseline risk scores, ward-first patients with COVID-19 ARDS had increased mortality and escalation to mechanical ventilation compared to ICU-direct patients. Ward-first patients requiring ICU upgrade within 48 h were at highest risk, highlighting a need for improved identification of this group at ED admission.
Keywords: COVID‐19; acute respiratory distress syndrome; disposition; emergency department.
© 2024 The Author(s). Journal of the American College of Emergency Physicians Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures
Similar articles
-
Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2017 Jul 13;7(7):CD004104. doi: 10.1002/14651858.CD004104.pub4. Cochrane Database Syst Rev. 2017. PMID: 28702957 Free PMC article.
-
Magnesium sulfate for acute exacerbations of chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2022 May 26;5(5):CD013506. doi: 10.1002/14651858.CD013506.pub2. Cochrane Database Syst Rev. 2022. PMID: 35616126 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Early spontaneous breathing for acute respiratory distress syndrome in individuals with COVID-19.Cochrane Database Syst Rev. 2022 Jun 29;6(6):CD015077. doi: 10.1002/14651858.CD015077. Cochrane Database Syst Rev. 2022. PMID: 35767435 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
References
-
- Prakash J, Bhattacharya PK, Yadav AK, Kumar A, Tudu LC, Prasad K. ROX index as a good predictor of high flow nasal cannula failure in COVID‐19 patients with acute hypoxemic respiratory failure: a systematic review and meta‐analysis. J Crit Care. 2021;66:102‐108. doi:10.1016/j.jcrc.2021.08.012 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous