

Clinical and surgical outcome in patients with cervical spondylodiscitis-a single-center retrospective case series of 24 patients
- PMID: 38887314
- PMCID: PMC11180735
- DOI: 10.3389/fsurg.2024.1292977
Clinical and surgical outcome in patients with cervical spondylodiscitis-a single-center retrospective case series of 24 patients
Abstract
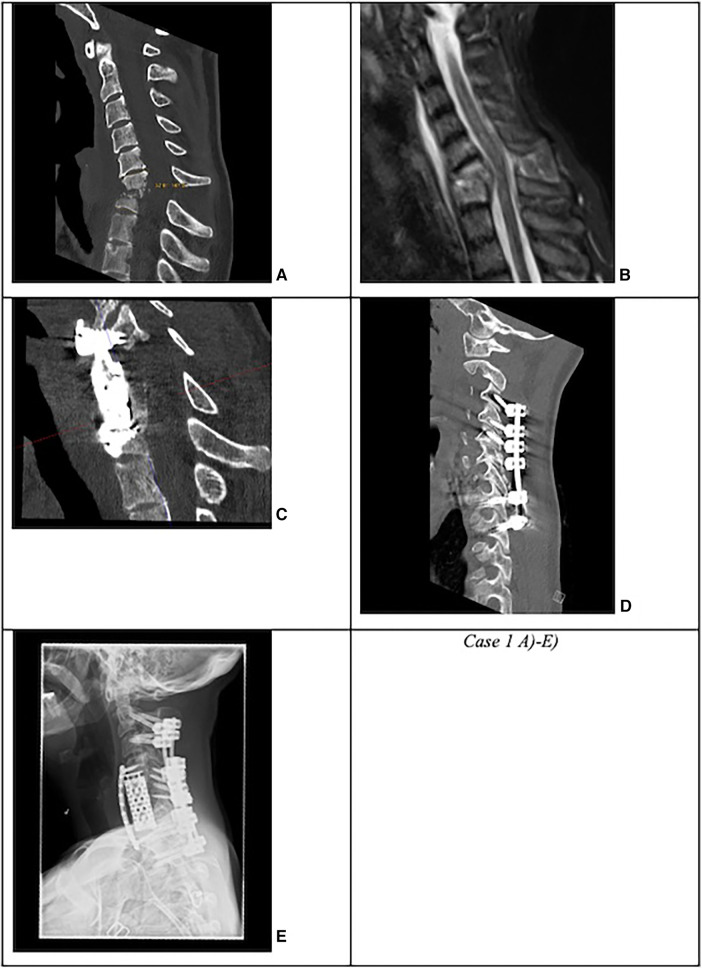
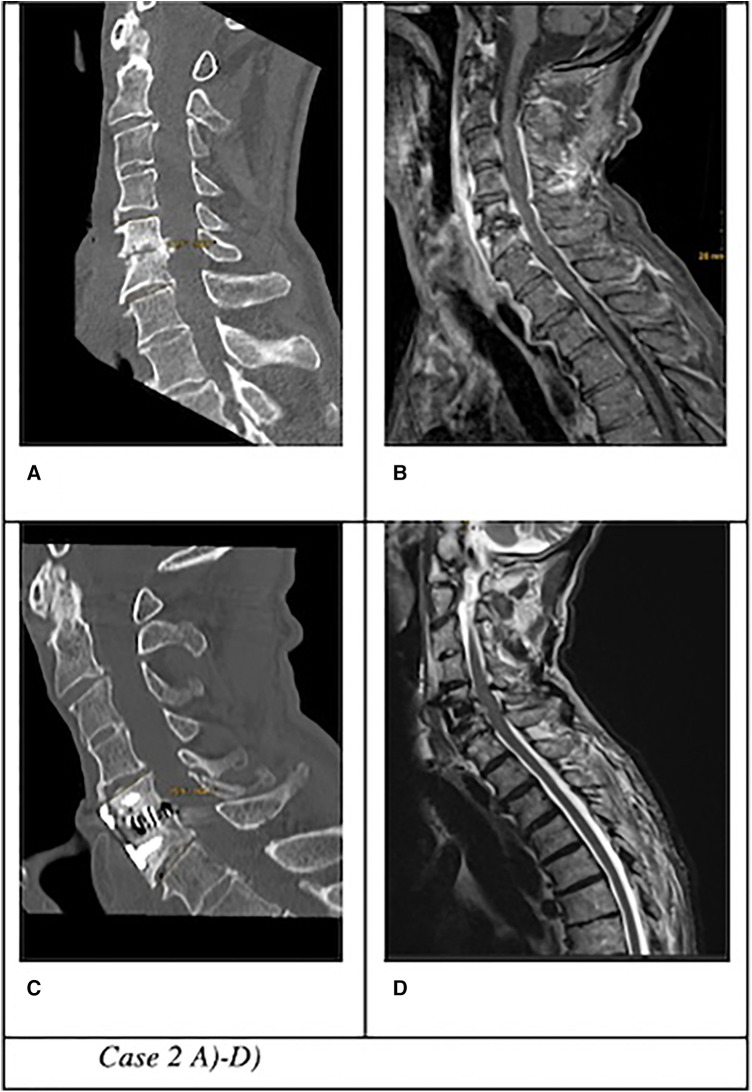
Objective: Cervical spondylodiscitis is a rare pathology, with an incidence of 0.5-2.5 per 100,000 population, posing significant potential risks. This type of infection can lead to neurological impairment in up to 29% of patients. Radical surgical debridement of the infected segment, fusion, and an intravenous antibiotic regimen remains the gold standard in most spine centers. This study aimed to analyze the surgical outcome in a tertiary spine center based on disease severity.
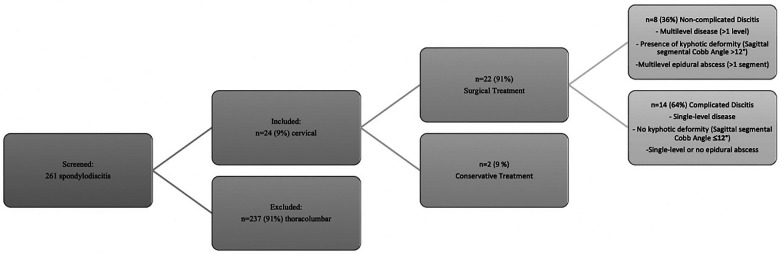
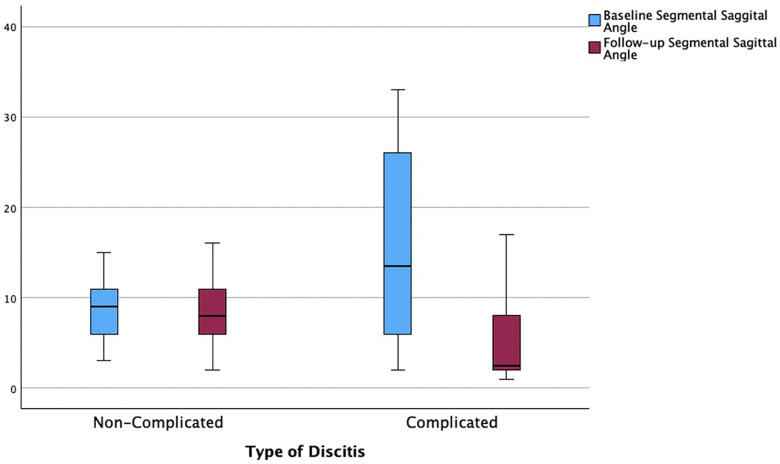
Methods: In this study, we retrospectively included all patients diagnosed with cervical spondylodiscitis and treated at the University Hospital Augsburg between January 2017 and May 2022. We collected and analyzed baseline parameters on clinical presentation with symptoms, laboratory parameters, radiological appearance, and surgical parameters such as type of approach and implant, as well as neurological and radiological outcomes. Descriptive statistics were performed using SPSS, and relevant correlations were examined using the t-test for independent samples and the chi-square test.
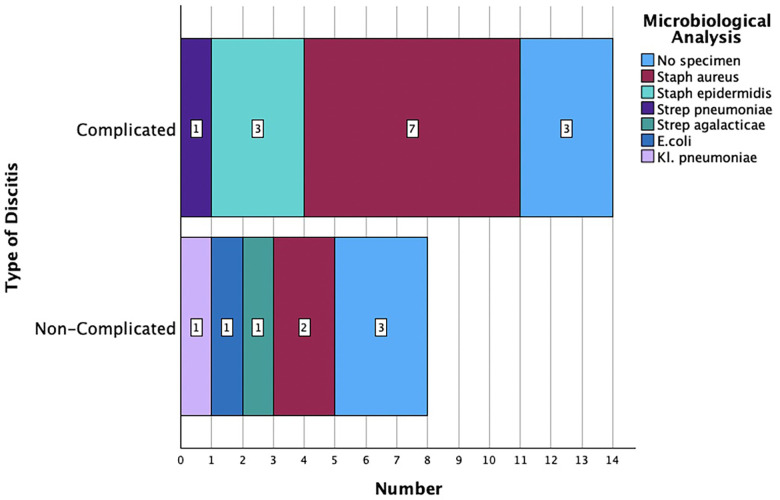
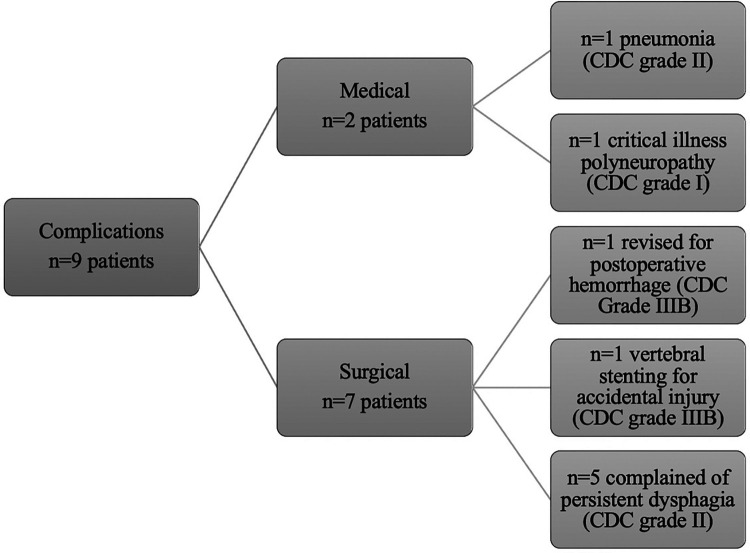
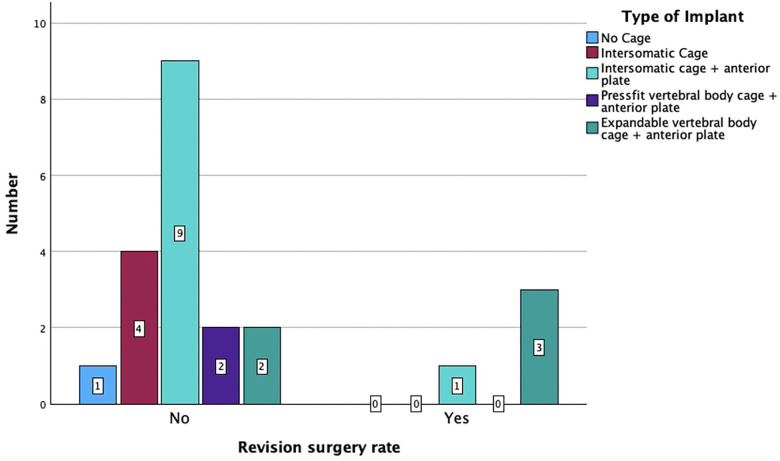
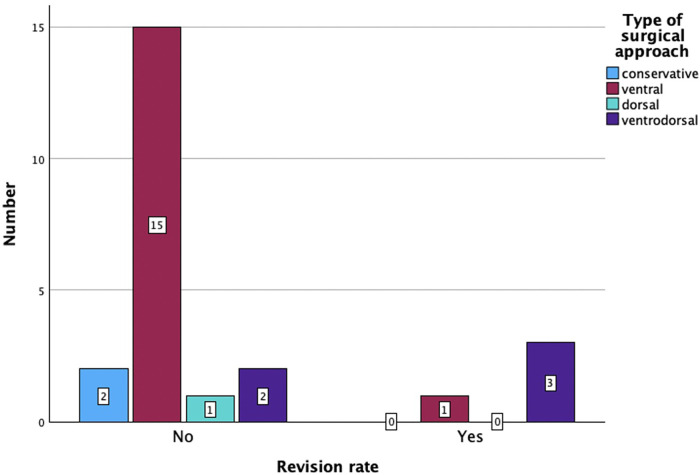
Results: Twenty-four patients (9%) with cervical spondylodiscitis were identified. Twenty-two (92%) surgically treated patients were subdivided into the complicated discitis group (n = 14, 64%) and the uncomplicated discitis group (n = 8, 36%). Seventeen patients (71%) presented with sepsis on admission, 17 patients (71%) were diagnosed with epidural abscess on primary imaging, and 5 patients (21%) had more than one discitis lesion at a distant spinal segment. The presence of epidural abscess was significantly associated with systemic sepsis (OR = 6.2; p = 0.03) and myelopathy symptoms (OR = 14.4; p = 0.00). The most frequently detected specimen was a multisensitive Staphylococcus aureus (10 patients, 42%). Six patients (25%) died after a median of 20 days despite antibiogram-accurate therapy, five of whom were diagnosed with a complicated type of discitis. The follow-up data of 15 patients (63%) revealed permanent neurological damage in 9 patients (38%). Notably, the surgical approach was a significant factor for revision surgery (p = 0.008), as three out of five (60%) ventrodorsal cases with complicated discitis were revised.
Conclusion: Cervical spondylodiscitis represents a severe infectious disease that is often associated with permanent neurological damage or a fatal outcome, despite adequate surgical and antibiotic treatments. Complicated types of discitis may require a more challenging surgical and clinical course.
Keywords: classification; discitis osteomyelitis; epidural abscess; sepsis; spinal; spondylodesis.
© 2024 Motov, Stemmer, Krauss, Bonk, Wolfert, Steininger, Shiban and Sommer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources