

Physical frailty, genetic predisposition, and the risks of severe non-alcoholic fatty liver disease and cirrhosis: a cohort study
- PMID: 38887910
- PMCID: PMC11294048
- DOI: 10.1002/jcsm.13506
Physical frailty, genetic predisposition, and the risks of severe non-alcoholic fatty liver disease and cirrhosis: a cohort study
Abstract
Background: Frailty, defined as a phenotype of decreased physiological reserves and diminished ability to respond to stressors, has been linked to the development of chronic diseases. Epidemiological evidence connecting frailty to non-alcoholic fatty liver disease (NAFLD) and cirrhosis risks remain sparse. We aimed to assess the longitudinal associations of frailty with the risks of severe NAFLD and cirrhosis in middle-aged to older adults and further explore the modification role of genetic risk on these associations.
Methods: This study included a total of 398 386 participants from the UK Biobank. Incident cases of severe NAFLD and cirrhosis were ascertained through linked hospital records and death registries. Frailty status was assessed by a modified version of the frailty phenotype, encompassing five key components: weight loss, tiredness, physical activity, gait speed, and grip strength. Participants were classified as pre-frailty if they met one or two of these criteria, and as frailty if they met three or more. Genetic predisposition to NAFLD and cirrhosis was estimated by genetic risk score (GRS) and further categorized into high, intermediate, and low genetic risk levels according to tertiles of GRSs. Cox proportional hazards regression model was employed to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for their associations.
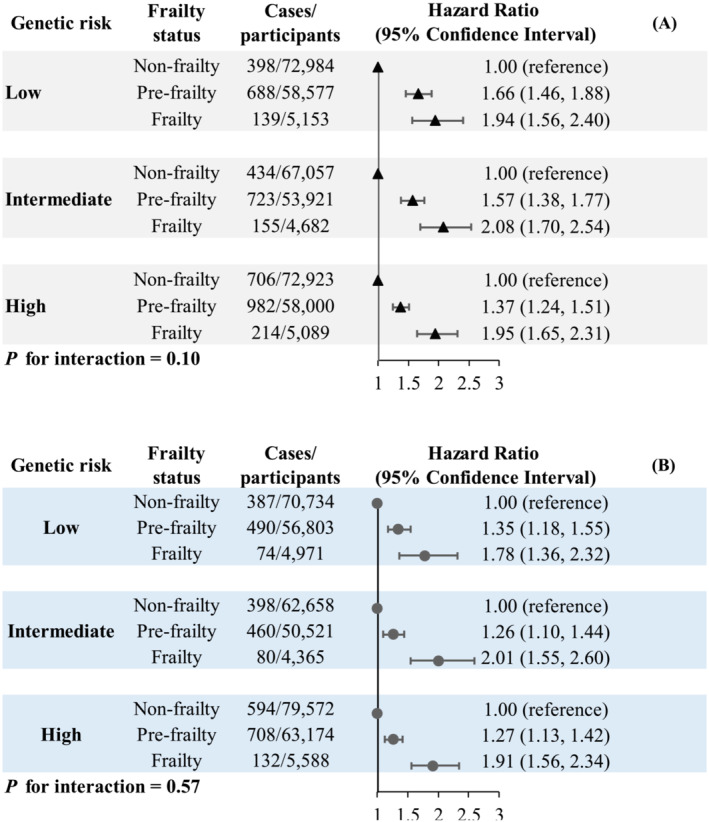
Results: The mean (standard deviation) age of the study population was 56.6 (8.03) years. 214 408 (53.8%) of the participants was female; 14 924 (3.75%) of participants met the criteria for frailty, 170 498 (42.8%) for pre-frailty, and 212 964 (53.5%) for non-frailty. Over a median follow-up of 12.0 years, we documented 4439 incident severe NAFLD and 3323 incident cirrhosis cases, respectively. Compared with non-frailty, both pre-frailty (HR: 1.50; 95% CI: 1.40-1.60) and frailty (HR: 1.98; 95% CI: 1.77-2.21) were associated with increased risk of NAFLD. Similar associations were observed for cirrhosis, the corresponding HRs (95% CIs) for non-frailty, pre-frailty, and frailty were 1.00 (reference), 1.29 (1.20, 1.38), and 1.90 (1.66, 2.18). Such associations were consistent across all genetic risk levels, with no observed interactions between frailty and GRSs (all P for interactions ≥0.10). Compared with participants with frailty and a low level of genetic risk, the greatest risk increasement in developing severe NAFLD (HR: 3.36; 95% CI: 2.83-3.99) and cirrhosis (HR: 2.81; 95% CI: 2.29-3.44) was both observed in those with frailty and a high level of genetic risk.
Conclusions: Our findings indicate that frailty is a significant predictor of severe NAFLD and cirrhosis, irrespective of genetic predisposition.
Keywords: Cirrhosis; Fatty liver; Frailty; Genetic predisposition; NAFLD.
© 2024 The Author(s). Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
None of the authors has any potential conflict of interest.
Figures
Similar articles
-
Intake of the different types of dairy products, genetic predisposition, and the risks of nonalcoholic fatty liver disease and cirrhosis: a prospective cohort study.Food Funct. 2024 May 7;15(9):5050-5062. doi: 10.1039/d3fo04602h. Food Funct. 2024. PMID: 38656457
-
Sleep patterns, genetic susceptibility, and risk of cirrhosis among individuals with nonalcoholic fatty liver disease.Hepatol Int. 2024 Aug;18(4):1158-1167. doi: 10.1007/s12072-024-10665-7. Epub 2024 Jun 18. Hepatol Int. 2024. PMID: 38888882
-
Physical frailty, genetic predisposition, and incident arrhythmias.J Cachexia Sarcopenia Muscle. 2024 Aug;15(4):1463-1472. doi: 10.1002/jcsm.13499. Epub 2024 Jun 9. J Cachexia Sarcopenia Muscle. 2024. PMID: 38853292 Free PMC article.
-
Frailty, genetic predisposition, and incident chronic kidney disease.Sci Rep. 2025 Apr 26;15(1):14625. doi: 10.1038/s41598-025-97280-0. Sci Rep. 2025. PMID: 40287467 Free PMC article.
-
The relationship between nonalcoholic fatty liver disease and frailty: A systematic review and meta-analysis.Diabetes Metab Syndr. 2025 Feb;19(2):103187. doi: 10.1016/j.dsx.2025.103187. Epub 2025 Jan 7. Diabetes Metab Syndr. 2025. PMID: 39798236
Cited by
-
Mapping of rehabilitation interventions and assessment methods for patients with liver cirrhosis: a scoping review.BMC Gastroenterol. 2025 Apr 23;25(1):291. doi: 10.1186/s12876-025-03881-4. BMC Gastroenterol. 2025. PMID: 40269747 Free PMC article.
References
-
- Younossi Z, Tacke F, Arrese M, Chander Sharma B, Mostafa I, Bugianesi E, et al. Global perspectives on nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology 2019;69:2672–2682. - PubMed
-
- Loomba R, Friedman SL, Shulman GI. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell 2021;184:2537–2564. - PubMed
-
- Cotter TG, Rinella M. Nonalcoholic fatty liver disease 2020: the state of the disease. Gastroenterology 2020;158:1851–1864. - PubMed
MeSH terms
Grants and funding
- 2021JH1/1040050/JieBangGuaShuai Project of Liaoning Province
- YESS20200151/Young Elite Scientists Sponsorship Program by China Association for Science and Technology
- M0294/345 Talent Project of Shengjing Hospital of China Medical University
- LJKMZ20221149/Scientific Research Project of Liaoning Province Education Department
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
