

Exposome-Wide Association Study of Body Mass Index Using a Novel Meta-Analytical Approach for Random Forest Models
- PMID: 38889167
- PMCID: PMC11218701
- DOI: 10.1289/EHP13393
Exposome-Wide Association Study of Body Mass Index Using a Novel Meta-Analytical Approach for Random Forest Models
Abstract
Background: Overweight and obesity impose a considerable individual and social burden, and the urban environments might encompass factors that contribute to obesity. Nevertheless, there is a scarcity of research that takes into account the simultaneous interaction of multiple environmental factors.
Objectives: Our objective was to perform an exposome-wide association study of body mass index (BMI) in a multicohort setting of 15 studies.
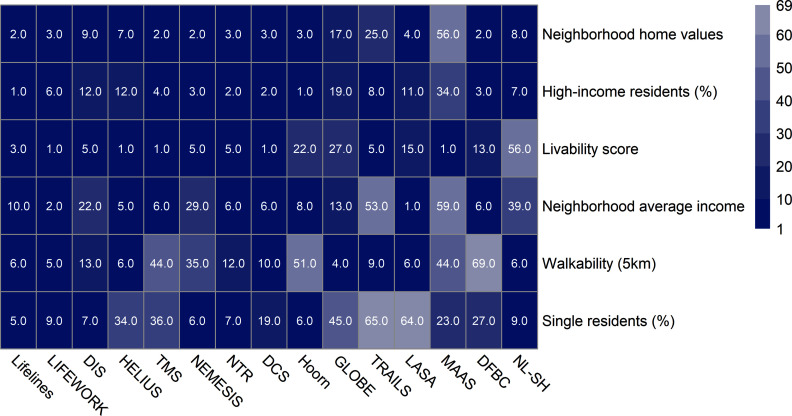
Methods: Studies were affiliated with the Dutch Geoscience and Health Cohort Consortium (GECCO), had different population sizes (688-141,825), and covered the entire Netherlands. Ten studies contained general population samples, others focused on specific populations including people with diabetes or impaired hearing. BMI was calculated from self-reported or measured height and weight. Associations with 69 residential neighborhood environmental factors (air pollution, noise, temperature, neighborhood socioeconomic and demographic factors, food environment, drivability, and walkability) were explored. Random forest (RF) regression addressed potential nonlinear and nonadditive associations. In the absence of formal methods for multimodel inference for RF, a rank aggregation-based meta-analytic strategy was used to summarize the results across the studies.
Results: Six exposures were associated with BMI: five indicating neighborhood economic or social environments (average home values, percentage of high-income residents, average income, livability score, share of single residents) and one indicating the physical activity environment (walkability in buffer area). Living in high-income neighborhoods and neighborhoods with higher livability scores was associated with lower BMI. Nonlinear associations were observed with neighborhood home values in all studies. Lower neighborhood home values were associated with higher BMI scores but only for values up to . The directions of associations were less consistent for walkability and share of single residents.
Discussion: Rank aggregation made it possible to flexibly combine the results from various studies, although between-study heterogeneity could not be estimated quantitatively based on RF models. Neighborhood social, economic, and physical environments had the strongest associations with BMI. https://doi.org/10.1289/EHP13393.
Figures


References
-
- WHO (World Health Organization). 2020. Obesity and Overweight. Geneva, Switzerland: WHO. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight [accessed 20 January 2021].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources