

Pre-emptive detection and evolution of relapse in acute myeloid leukemia by flow cytometric measurable residual disease surveillance
- PMID: 38890448
- PMCID: PMC11286513
- DOI: 10.1038/s41375-024-02300-z
Pre-emptive detection and evolution of relapse in acute myeloid leukemia by flow cytometric measurable residual disease surveillance
Abstract
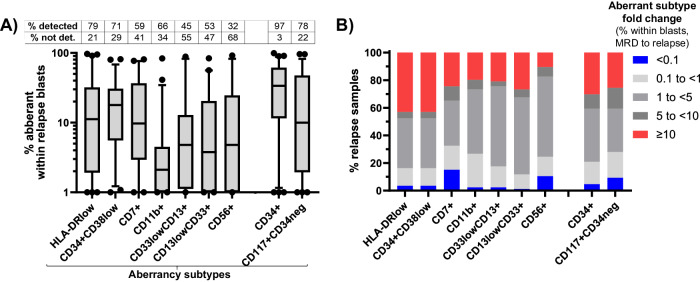
Measurable residual disease (MRD) surveillance in acute myeloid leukemia (AML) may identify patients destined for relapse and thus provide the option of pre-emptive therapy to improve their outcome. Whilst flow cytometric MRD (Flow-MRD) can be applied to high-risk AML/ myelodysplasia patients, its diagnostic performance for detecting impending relapse is unknown. We evaluated this in a cohort comprising 136 true positives (bone marrows preceding relapse by a median of 2.45 months) and 155 true negatives (bone marrows during sustained remission). At an optimal Flow-MRD threshold of 0.040%, clinical sensitivity and specificity for relapse was 74% and 87% respectively (51% and 98% for Flow-MRD ≥ 0.1%) by 'different-from-normal' analysis. Median relapse kinetics were 0.78 log10/month but significantly higher at 0.92 log10/month for FLT3-mutated AML. Computational (unsupervised) Flow-MRD (C-Flow-MRD) generated optimal MRD thresholds of 0.036% and 0.082% with equivalent clinical sensitivity to standard analysis. C-Flow-MRD-identified aberrancies in HLADRlow or CD34+CD38low (LSC-type) subpopulations contributed the greatest clinical accuracy (56% sensitivity, 90% specificity) and notably, by longitudinal profiling expanded rapidly within blasts in > 40% of 86 paired MRD and relapse samples. In conclusion, flow MRD surveillance can detect MRD relapse in high risk AML and its evaluation may be enhanced by computational analysis.
© 2024. The Author(s).
Conflict of interest statement
NM, FD, AP, CR, GA, SG, AA, MJ, and AP, have no conflicts to declare. SDF declares research funding from Jazz and BMS; Speakers Bureau with Jazz, Pfizer and Novartis; advisory committee with MPAACT. CH and GG, The National Heart, Lung, and Blood Institute receives research funding for the laboratory of Dr. Hourigan from the Foundation of the NIH AML MRD Biomarkers Consortium.
Figures


References
-
- Heuser M, Freeman SD, Ossenkoppele GJ, Buccisano F, Hourigan CS, Ngai LL, et al. 2021 Update on Measurable Residual Disease (MRD) in Acute Myeloid Leukemia (AML): A Consensus Document from the European LeukemiaNet MRD Working Party. Blood. 2021;138:2753–67. 10.1182/blood.2021013626 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
