

Impact of commissural calcification on clinical outcome of percutaneous balloon mitral valvuloplasty; a retrospective cohort study of 876 patients
- PMID: 38890637
- PMCID: PMC11184739
- DOI: 10.1186/s12872-024-03932-w
Impact of commissural calcification on clinical outcome of percutaneous balloon mitral valvuloplasty; a retrospective cohort study of 876 patients
Abstract
Background: Percutaneous balloon mitral valvuloplasty (PBMV) is the ACC/AHA class I recommendation for treating symptomatic rheumatic mitral stenosis with suitable valve morphology, less than moderate MR and absence of left atrium clot. The mitral valve restenosis and significant mitral regurgitation (MR) are known adverse outcomes of PBMV. This study aimed to evaluate the outcomes of PBMV in patients with severe mitral stenosis and the effect of Commissural Calcification (CC) on the outcomes.
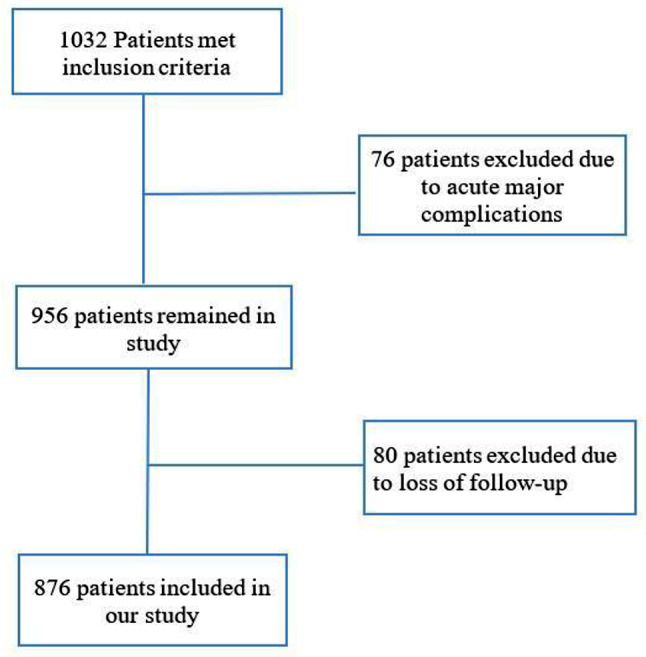
Methods: In this single-center retrospective cohort study, 876 patients who underwent PBMV were categorized into three groups based on their Wilkins score (Group I: score ≤ 8, Group II: score 9-10, and Group III: score 11-12). Patients were evaluated before, early after PBMV and at 6- and 24-month follow-ups. Main clinical outcomes were defined as significant restenosis and or symptomatic significant MR (moderate to severe and severe MR) or candidate for mitral valve replacement (MVR). The outcomes were compared between patients with and without CC.
Results: A total of 876 patients with mean age 46.4 ± 12.3 years (81.0% females) were categorized based on Wilkins score. 333 (38.0%) were in Group I, 501 (57.2%) were in Group II, and 42 (4.8%) were in Group III. CC was present in 175 (20.0%) of the patients, among whom 95 (54.3%) had calcification of the anterolateral commissure, 64 (36.6%) had calcification of the posteromedial commissure, and in 16 (9.1%) patients both commissures were calcified. There was a significant difference in Wilkins score between patients with and without CC (P < 0.001). CC was associated with higher odds of significant symptomatic MR at early and mid-term follow up (OR: 1.69, 95%CI 1.19-2.41, P = 0.003; and OR: 3.90, 95%CI 2.61-5.83, P < 0.001, respectively), but not with restenosis (P = 0.128). Wilkins Groups II and III did not show higher odds of significant symptomatic MR compared to Group I at early (II: P = 0.784; III: P = 0.098) and mid-term follow up (II: P = 0.216; III: P = 0.227). Patients in Wilkins Group II had higher odds of restenosis compared to Group I (OR: 2.96,95%CI: 1.35-6.27, P = 0.007).
Conclusion: Commissural calcification (CC) is an independent predictor of the significant symptomatic MR (an important determinant of adverse outcome) following PBMV in the early and mid-term follow-up. Mitral valve restenosis occurs more in patients with higher Wilkins score compared to group I with score ≤ 8. Combined Wilkins score and CC should be considered for patient suitability for PBMV.
Keywords: Commissure calcification; Mitral Stenosis; Mitral valve; Percutaneous balloon mitral valvuloplasty (PBMV); Rheumatic Valve Disease.
© 2024. The Author(s).
Conflict of interest statement
The authors of this paper declare no competing interest.
Figures



References
-
- Padmavati S. Rheumatic fever and rheumatic heart disease in India at the turn of the century. Indian Heart J. 2001;53(1):35–7. - PubMed
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, III, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice guidelines. J Am Coll Cardiol. 2021;77(4):450–500. doi: 10.1016/j.jacc.2020.11.035. - DOI - PubMed
-
- Iung B, Garbarz E, Michaud P, Helou S, Farah B, Berdah P, et al. Late results of percutaneous mitral commissurotomy in a series of 1024 patients: analysis of late clinical deterioration: frequency, anatomic findings, and predictive factors. Circulation. 1999;99(25):3272–8. doi: 10.1161/01.CIR.99.25.3272. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
