

Treating sleep-disordered breathing of idiopathic pulmonary fibrosis patients with CPAP and nocturnal oxygen treatment. A pilot study : Sleep-disordered breathing treatment in IPF
- PMID: 38890648
- PMCID: PMC11186220
- DOI: 10.1186/s12931-024-02871-6
Treating sleep-disordered breathing of idiopathic pulmonary fibrosis patients with CPAP and nocturnal oxygen treatment. A pilot study : Sleep-disordered breathing treatment in IPF
Abstract
Introduction: Sleep-disordered breathing (SDB) is a major comorbidity in idiopathic pulmonary fibrosis (IPF) and is associated with a poor outcome. There is a lack of knowledge regarding the impact of SDB treatment on IPF. We assessed at one year: (1) the effect of CPAP and/or nocturnal oxygen therapy on IPF regarding lung function, blood mediators, and quality of life; (2) adherence to SDB treatment and SDB changes.
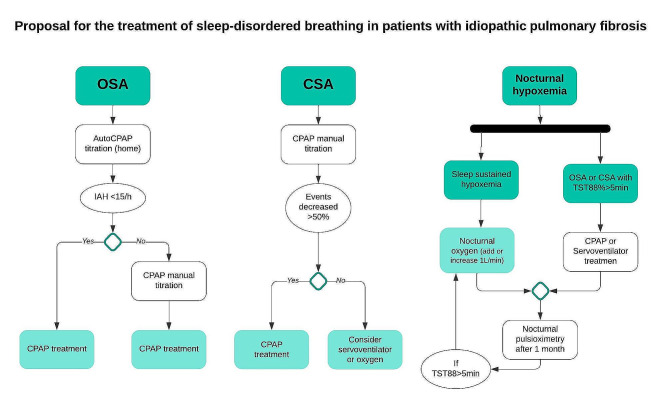
Methodology: This is a prospective study of consecutive newly diagnosed IPF patients initiating anti-fibrotic treatment. Lung function, polysomnography, blood tests and quality of life questionnaires were performed at inclusion and after one year. Patients were classified as obstructive sleep apnoea (OSA), central sleep apnoea (CSA), and sleep-sustained hypoxemia (SSH). SDB therapy (CPAP and/or nocturnal oxygen therapy) was initiated if needed.
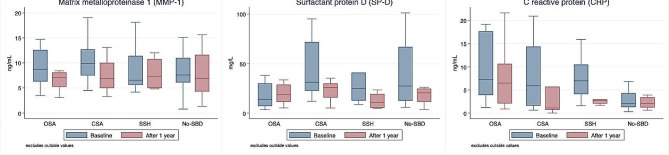
Results: Fifty patients were enrolled (36% had OSA, 22% CSA, and 12% SSH). CPAP was started in 54% of patients and nocturnal oxygen therapy in 16%. At one-year, polysomnography found improved parameters, though 17% of patients had to add nocturnal oxygen therapy or CPAP, while 33% presented SDB onset at this second polysomnography. CPAP compliance at one year was 6.74 h/night (SD 0.74). After one year, matrix metalloproteinase-1 decreased in OSA and CSA (p = 0.029; p = 0.027), C-reactive protein in OSA (p = 0.045), and surfactant protein D in CSA group (p = 0.074). There was no significant change in lung function.
Conclusions: Treatment of SBD with CPAP and NOT can be well tolerated with a high compliance. IPF patients may exhibit SDB progression and require periodic re-assessment. Further studies to evaluate the impact of SDB treatment on lung function and serological mediators are needed.
Keywords: Apnoea; Biomarkers; CPAP; Hypoxemia; Idiopathic pulmonary fibrosis; Sleep; Supplemental oxygen therapy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors state that they have no conflict of interests to declare.
Figures
Similar articles
-
Obstructive sleep apnea should be treated in patients with idiopathic pulmonary fibrosis.Sleep Breath. 2015 Mar;19(1):385-91. doi: 10.1007/s11325-014-1033-6. Epub 2014 Jul 16. Sleep Breath. 2015. PMID: 25028171 Clinical Trial.
-
CPAP therapy in patients with idiopathic pulmonary fibrosis and obstructive sleep apnea: does it offer a better quality of life and sleep?Sleep Breath. 2013 Dec;17(4):1137-43. doi: 10.1007/s11325-013-0813-8. Epub 2013 Feb 6. Sleep Breath. 2013. PMID: 23386371
-
Quality of life in idiopathic pulmonary fibrosis: The impact of sleep disordered breathing.Respir Med. 2019 Feb;147:51-57. doi: 10.1016/j.rmed.2018.12.018. Epub 2019 Jan 10. Respir Med. 2019. PMID: 30704699
-
Sleep and breathing in idiopathic pulmonary fibrosis.J Physiol Pharmacol. 2009 Nov;60 Suppl 5:13-4. J Physiol Pharmacol. 2009. PMID: 20134032 Review.
-
Recognition and treatment of sleep-disordered breathing: an important component of chronic disease management.J Transl Med. 2017 May 25;15(1):114. doi: 10.1186/s12967-017-1211-y. J Transl Med. 2017. PMID: 28545542 Free PMC article. Review.
Cited by
-
Treatable traits in interstitial lung disease: a narrative review.Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251335774. doi: 10.1177/17534666251335774. Epub 2025 May 3. Ther Adv Respir Dis. 2025. PMID: 40317250 Free PMC article. Review.
-
The Link Between Sleep-Related Breathing Disorders and Idiopathic Pulmonary Fibrosis: Pathophysiological Mechanisms and Treatment Options-A Review.J Clin Med. 2025 Mar 24;14(7):2205. doi: 10.3390/jcm14072205. J Clin Med. 2025. PMID: 40217656 Free PMC article. Review.
References
-
- Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Inoue Y, Johkoh T, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2022;205(9):e18–47. doi: 10.1164/rccm.202202-0399ST. - DOI - PMC - PubMed
-
- Platenburg M, van Moorsel CHM, Wiertz IA, van der Vis JJ, Vorselaars ADM, Veltkamp M et al. Improved Survival of IPF patients Treated With Antifibrotic Drugs Compared With Untreated Patients. Lung. 2023. - PubMed
Publication types
MeSH terms
Grants and funding
- CM20/00093 and PMP22/00083/Instituto de Salud Carlos III
- CM20/00093 and PMP22/00083/Instituto de Salud Carlos III
- 631/2018; 685/2018; and Emerging ILD Group of SEPAR grant 005/Sociedad Española de Neumología y Cirugía Torácica
- 631/2018; 685/2018; and Emerging ILD Group of SEPAR grant 005/Sociedad Española de Neumología y Cirugía Torácica
- grant 2019/Sociedad Española Del Sueño
LinkOut - more resources
Full Text Sources
Medical
Research Materials
