

The Effect of Adult Smoking Behavior on Children's Exposure to Secondhand Smoke. An Analysis Based on Salivary Cotinine Levels Among Children in Dhaka and Karachi
- PMID: 38890774
- PMCID: PMC11494616
- DOI: 10.1093/ntr/ntae130
The Effect of Adult Smoking Behavior on Children's Exposure to Secondhand Smoke. An Analysis Based on Salivary Cotinine Levels Among Children in Dhaka and Karachi
Abstract
Introduction: Exposure to secondhand smoke (SHS) risks children's health. However, biomarkers are rarely used to study SHS exposure among children in low- and middle-income countries.
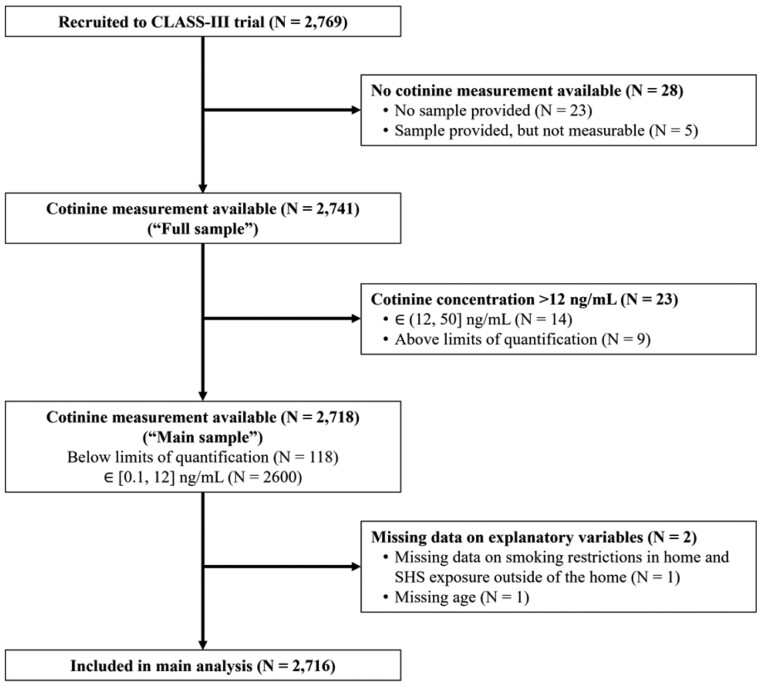
Aims and methods: We analyzed cross-sectional data collected between March and November 2022 for a cluster-randomized controlled trial investigating a Smoke-Free Intervention in 2769 children aged 9-15 in 74 schools (34 in Dhaka, Bangladesh, and 40 in Karachi, Pakistan). Children's saliva was tested for the concentration of cotinine-a highly sensitive and specific biomarker for SHS exposure. Based on their reports, children's homes were categorized as Nonsmoking Homes (NSH) when residents were nonsmokers; Smoke-free Homes (SFH) when residents and visitors smoked outdoors only; and Smoke-permitted Homes (SPH) when either residents or visitors smoked indoors. We compared cotinine concentrations across these home types and the two cities using a proportional odds model.
Results: Overall, 95.7% of children (92% in Dhaka; and 99.4% in Karachi) had cotinine levels between 0.1 and 12 ng/mL, indicating SHS exposure. Median cotinine levels were higher in Karachi (0.58 ng/mL, IQR 0.37 to 0.93) than in Dhaka (0.27 ng/mL, IQR 0.16 to 0.49). Median cotinine concentration was also higher among children living in SPH than those in either NSH or SFH; with absolute differences of approximately 0.1-0.3 and 0.05 ng/mL, respectively.
Conclusions: The level of SHS exposure in Dhaka and Karachi indicates widespread and unrestricted smoking. Smoking restrictions in households and enforcement of smoking bans are urgently needed.
Implications: The high levels of SHS exposure in children living in SFH suggest parental behavior to hide their smoking and/or exposure in private vehicles or public spaces. It is important to advocate for SFH and cars to protect children from SHS exposure. However, these initiatives alone may not be enough. There is a need to enforce smoking bans in enclosed public places and transportation, as well as extend these bans to playgrounds, parks, fairgrounds, and other public spaces that children frequently visit. It is essential to complement smoking restrictions with tobacco cessation advice and support in these settings.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Research on Nicotine and Tobacco.
Conflict of interest statement
All authors declared there is no conflict of interest.
Figures


References
-
- Alla F. Second-hand tobacco exposure in children: evidence for action. Lancet Public Health. 2021;6(8):e537–e538. - PubMed
-
- Ma C, Heiland EG, Li Z, et al. Global trends in the prevalence of secondhand smoke exposure among adolescents aged 12-16 years from 1999 to 2018: an analysis of repeated cross-sectional surveys. Lancet Glob Health. 2021;9(12):e1667–e1678. - PubMed
-
- Jones LL, Hassanien A, Cook DG, Britton J, Leonardi-Bee J.. Parental smoking and the risk of middle ear disease in children: a systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2012;166(1):18–27. - PubMed
-
- GBD Compare. Institute for Health Metrics and Evaluation. http://vizhub.healthdata.org/gbd-compare (Accessed October 31, 2023).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
