

Many Faces of Regulatory T Cells: Heterogeneity or Plasticity?
- PMID: 38891091
- PMCID: PMC11171907
- DOI: 10.3390/cells13110959
Many Faces of Regulatory T Cells: Heterogeneity or Plasticity?
Abstract
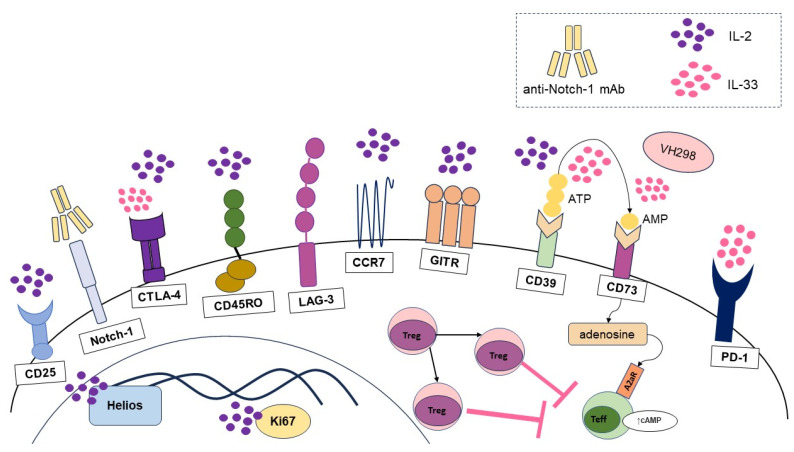
Regulatory T cells (Tregs) are essential for maintaining the immune balance in normal and pathological conditions. In autoimmune diseases and transplantation, they restrain the loss of self-tolerance and promote engraftment, whereas in cancer, an increase in Treg numbers is mostly associated with tumor growth and poor prognosis. Numerous markers and their combinations have been used to identify Treg subsets, demonstrating the phenotypic diversity of Tregs. The complexity of Treg identification can be hampered by the unstable expression of some markers, the decrease in the expression of a specific marker over time or the emergence of a new marker. It remains unclear whether such phenotypic shifts are due to new conditions or whether the observed changes are due to initially different populations. In the first case, cellular plasticity is observed, whereas in the second, cellular heterogeneity is observed. The difference between these terms in relation to Tregs is rather blurred. Considering the promising perspectives of Tregs in regenerative cell-based therapy, the existing confusing data on Treg phenotypes require further investigation and analysis. In our review, we introduce criteria that allow us to distinguish between the heterogeneity and plasticity of Tregs normally and pathologically, taking a closer look at their diversity and drawing the line between two terms.
Keywords: heterogeneity; phenotype switch; plasticity; regulatory T cells; treg-based therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Regulatory T Cell Plasticity and Stability and Autoimmune Diseases.Clin Rev Allergy Immunol. 2020 Feb;58(1):52-70. doi: 10.1007/s12016-018-8721-0. Clin Rev Allergy Immunol. 2020. PMID: 30449014 Review.
-
Defining Human Regulatory T Cells beyond FOXP3: The Need to Combine Phenotype with Function.Cells. 2024 May 30;13(11):941. doi: 10.3390/cells13110941. Cells. 2024. PMID: 38891073 Free PMC article. Review.
-
Human Regulatory T Cells From Umbilical Cord Blood Display Increased Repertoire Diversity and Lineage Stability Relative to Adult Peripheral Blood.Front Immunol. 2020 Apr 15;11:611. doi: 10.3389/fimmu.2020.00611. eCollection 2020. Front Immunol. 2020. PMID: 32351504 Free PMC article.
-
Molecular Insights Into Regulatory T-Cell Adaptation to Self, Environment, and Host Tissues: Plasticity or Loss of Function in Autoimmune Disease.Front Immunol. 2020 Sep 15;11:1269. doi: 10.3389/fimmu.2020.01269. eCollection 2020. Front Immunol. 2020. PMID: 33072063 Free PMC article. Review.
-
Atherosclerosis-Driven Treg Plasticity Results in Formation of a Dysfunctional Subset of Plastic IFNγ+ Th1/Tregs.Circ Res. 2016 Nov 11;119(11):1190-1203. doi: 10.1161/CIRCRESAHA.116.309764. Epub 2016 Sep 15. Circ Res. 2016. PMID: 27635087 Free PMC article.
Cited by
-
Immunosuppressive mechanisms and therapeutic targeting of regulatory T cells in ovarian cancer.Front Immunol. 2025 Jul 9;16:1631226. doi: 10.3389/fimmu.2025.1631226. eCollection 2025. Front Immunol. 2025. PMID: 40703514 Free PMC article. Review.
-
Mini-Review: Tregs as a Tool for Therapy-Obvious and Non-Obvious Challenges and Solutions.Cells. 2024 Oct 11;13(20):1680. doi: 10.3390/cells13201680. Cells. 2024. PMID: 39451198 Free PMC article. Review.
-
Investigating the Genetic Links Between Immune Cell Profiles and Bladder Cancer: A Multidisciplinary Bioinformatics Approach.Biomedicines. 2025 May 15;13(5):1203. doi: 10.3390/biomedicines13051203. Biomedicines. 2025. PMID: 40427030 Free PMC article.
References
-
- Todo S., Yamashita K., Goto R., Zaitsu M., Nagatsu A., Oura T., Watanabe M., Aoyagi T., Suzuki T., Shimamura T., et al. A Pilot Study of Operational Tolerance with a Regulatory T-Cell-Based Cell Therapy in Living Donor Liver Transplantation. Hepatology. 2016;64:632–643. doi: 10.1002/HEP.28459. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
