

Risk Factors for Progression of Cervical Congenital Scoliosis and Associated Compensatory Curve Behavior
- PMID: 38892749
- PMCID: PMC11172909
- DOI: 10.3390/jcm13113039
Risk Factors for Progression of Cervical Congenital Scoliosis and Associated Compensatory Curve Behavior
Abstract
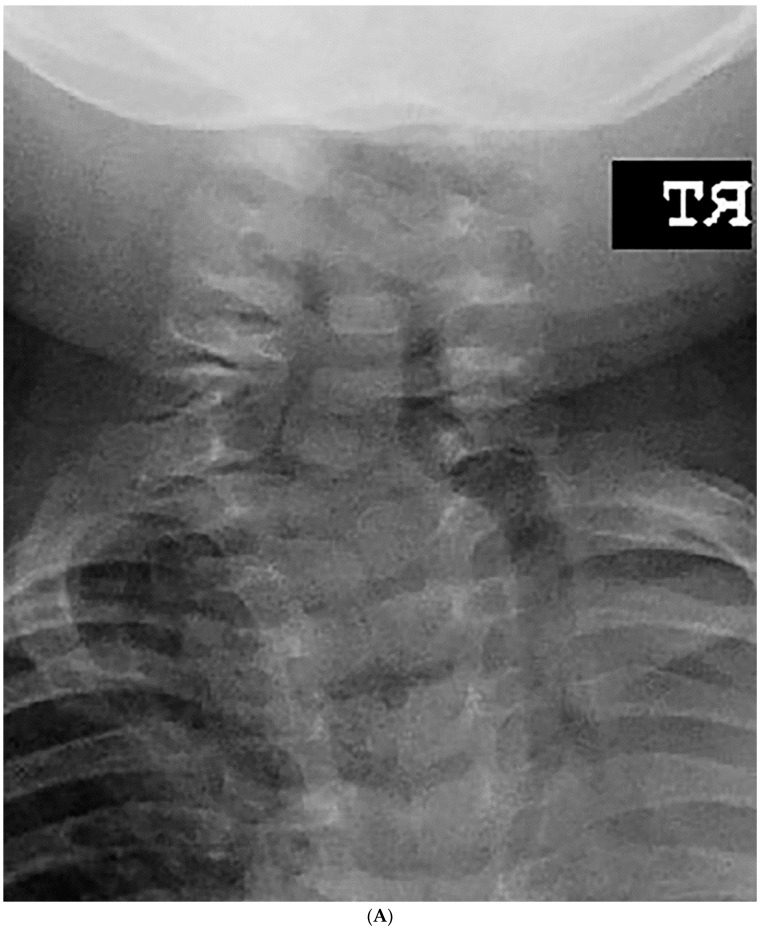
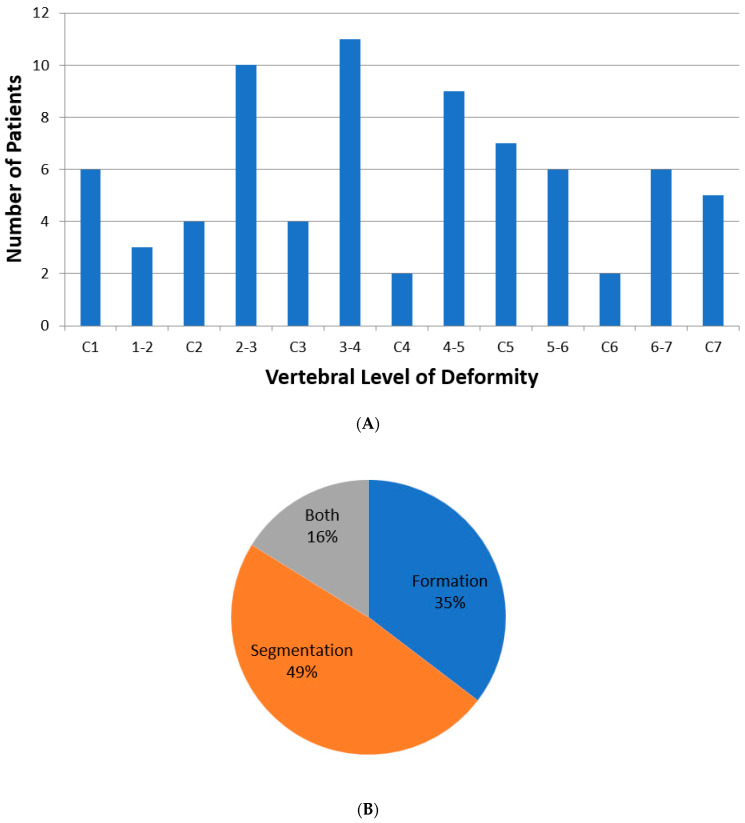
Background: This study investigated risk factors for progression of deformity in pediatric congenital cervical scoliosis (CCS) and evaluated the correlation between congenital cervical curves and compensatory thoracic and lumbar curves. Methods: Medical records were retrospectively reviewed for 38 pediatric patients with CCS with a minimum 2-year follow-up. Curve progression was defined as >10° increase in cervical coronal curve angle between presentation and last follow-up. Results: A total of 38 patients (16 girls, 22 boys) with a mean age at presentation of 5.6 ± 4.1 years met the inclusion criteria. Sixteen patients (42%) had curve progression with a mean follow-up of 3.1 ± 3.0 years. At presentation, T1 slope was significantly larger among children with progressive deformities (p = 0.041). A total of 18 of the 38 patients with strictly cervical spine deformity were then selected for subanalysis to evaluate the progression of compensatory curves. Cervical major coronal curves were found to significantly correlate with lumbar major coronal curves (r = 0.409), C2 central sacral vertical line (CSVL) (r = 0.407), and C7-CSVL (r = 0.403) (p < 0.05). Thoracic major coronal curves did not significantly correlate with cervical major coronal curves (r = 0.218) (p > 0.05). Conclusion: In conclusion, 42% of osseous CCS curves progressed over time in the overall cohort, and high initial T1 slope was found to be most highly correlated with progression of cervical deformity. Cervical major coronal curves significantly correlated with lumbar curve magnitude but not with thoracic curve size in isolated CCS, possibly due to the increased flexibility of the lumbar spine which may allow greater compensatory balance and thus have a greater correlation with cervical curve magnitude and possibly progression.
Keywords: cervical spine deformity; compensatory curve; congenital cervical scoliosis; pediatric scoliosis; risk factors; secondary curve.
Conflict of interest statement
A. F. Samdani: Paid consultant DePuy Synthes Spine, Ethicon, Globus NuVasive, Medical Device Business Services, Mirus, Orthofix, Stryker, ZimVie; Royalties Globus NuVasive, ZimVie
Figures









Similar articles
-
The effectiveness of selective thoracic fusion for treating adolescent idiopathic scoliosis: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):4-16. doi: 10.11124/jbisrir-2015-2338. JBI Database System Rev Implement Rep. 2015. PMID: 26657460
-
Evaluation of a combined approach to the correction of congenital cervical or cervicothoracic scoliosis.Spine J. 2019 May;19(5):803-815. doi: 10.1016/j.spinee.2018.11.006. Epub 2018 Nov 15. Spine J. 2019. PMID: 30447326
-
Thoracolumbar curve behavior after selective thoracic anterior vertebral body tethering in Lenke 1A vs Lenke 1C curve patterns.Spine Deform. 2023 Jul;11(4):897-907. doi: 10.1007/s43390-023-00664-3. Epub 2023 Mar 9. Spine Deform. 2023. PMID: 36892744 Free PMC article.
-
Analysis of the cervical spine sagittal alignment in young idiopathic scoliosis: a morphological classification of 120 cases.Eur Spine J. 2013 Nov;22(11):2372-81. doi: 10.1007/s00586-013-2753-1. Epub 2013 Apr 12. Eur Spine J. 2013. PMID: 23580056 Free PMC article. Review.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
Cited by
-
Spinal sagittal and coronal morphology characteristics in children with short stature.Quant Imaging Med Surg. 2025 Feb 1;15(2):1383-1395. doi: 10.21037/qims-24-992. Epub 2025 Jan 22. Quant Imaging Med Surg. 2025. PMID: 39995716 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
