

Guideline-Optimised Treatment in Heart Failure-Do Higher Doses Reduce Systemic Inflammation More Significantly?
- PMID: 38892766
- PMCID: PMC11173071
- DOI: 10.3390/jcm13113056
Guideline-Optimised Treatment in Heart Failure-Do Higher Doses Reduce Systemic Inflammation More Significantly?
Abstract
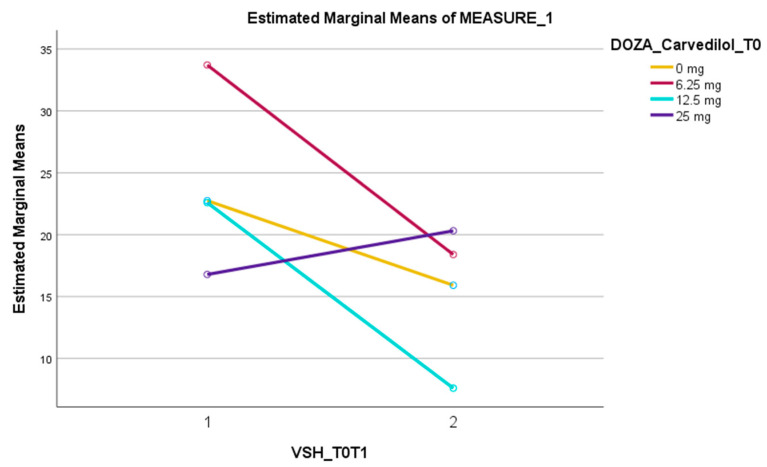
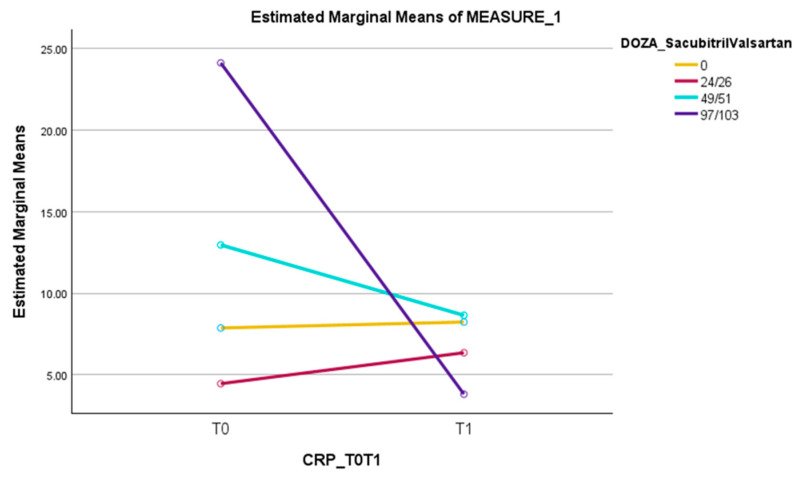
Background: Chronic inflammation is a constant phenomenon which accompanies the heart failure pathophysiology. In all phenotypes of heart failure, irrespective of the ejection fraction, there is a permanent low-grade activation and synthesis of proinflammatory cytokines. Many classes of anti-remodelling medication used in the treatment of chronic heart failure have been postulated to have an anti-inflammatory effect. Methods: This retrospective study enrolled 220 patients and focused on evaluating the effect of the most used active substances from these classes in reducing the level of inflammatory biomarkers (C reactive protein, erythrocyte sedimentation rate and fibrinogen) after initiation or up-titration. Our research is evaluating if this anti-inflammatory effect intensifies while raising the dose. The evaluation was performed at two visits with an interval between them of 6 months. Results: From the beta-blockers class, carvedilol showed a reduction in erythrocyte sedimentation rate (ESR), in low (6.25 mg, bi daily) and medium (12.5 mg, bi daily) doses. At the same time, sacubitril/valsartan showed a reduction in CRP levels. This effect was obtained only in the medium (49/51 mg, bi daily) and high (97/103 mg, bi daily) doses, with the maximum reduction being observed in the high dose. Conclusions: From the classes of medication evaluated, the study showed a significant reduction in ESR levels in the low and medium doses of carvedilol and a reduction in CRP values in the cases of medium and high doses of ARNI.
Keywords: ACE-I; ARB; ARNI; CRP; ESR; MRA; SGLT2i; beta-blockers; fibrinogen; heart failure; inflammation; left ventricular ejection fraction.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Titration of Medical Therapy for Heart Failure With Reduced Ejection Fraction.J Am Coll Cardiol. 2019 May 21;73(19):2365-2383. doi: 10.1016/j.jacc.2019.02.015. Epub 2019 Mar 4. J Am Coll Cardiol. 2019. PMID: 30844480 Free PMC article.
-
C-reactive protein reduction with sacubitril-valsartan treatment in heart failure patients.Am J Cardiovasc Dis. 2020 Aug 15;10(3):174-181. eCollection 2020. Am J Cardiovasc Dis. 2020. PMID: 32923098 Free PMC article.
-
Our Experience With Sacubitril/Valsartan in Chronic Heart Failure Management - HFrEF in the Ambulatory Setting.Med Arch. 2022 Apr;76(2):101-107. doi: 10.5455/medarh.2022.76.101-107. Med Arch. 2022. PMID: 35774049 Free PMC article.
-
Angiotensin Receptor Neprilysin Inhibition in Heart Failure With Preserved Ejection Fraction: Rationale and Design of the PARAGON-HF Trial.JACC Heart Fail. 2017 Jul;5(7):471-482. doi: 10.1016/j.jchf.2017.04.013. Epub 2017 Jun 26. JACC Heart Fail. 2017. PMID: 28662936 Review.
-
Effects of sacubitril-valsartan on heart failure patients with mid-range ejection fractions: A systematic review and meta-analysis.Front Pharmacol. 2022 Oct 24;13:982372. doi: 10.3389/fphar.2022.982372. eCollection 2022. Front Pharmacol. 2022. PMID: 36353496 Free PMC article. Review.
Cited by
-
Remote Monitoring of Patients with Heart Failure: Characteristics of Effective Programs and Implementation Strategies.Vasc Health Risk Manag. 2025 Jun 25;21:489-503. doi: 10.2147/VHRM.S521952. eCollection 2025. Vasc Health Risk Manag. 2025. PMID: 40585898 Free PMC article.
-
Effects of anti-inflammatory therapy in acute heart failure: a systematic review and meta-analysis.Heart Fail Rev. 2025 May;30(3):575-587. doi: 10.1007/s10741-025-10491-5. Epub 2025 Feb 12. Heart Fail Rev. 2025. PMID: 39939545
-
The real-world anti-inflammatory effect of SGLT2i in patients with chronic heart failure.J Med Life. 2025 Feb;18(2):155-164. doi: 10.25122/jml-2025-0011. J Med Life. 2025. PMID: 40134442 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
