

Partial Deployment to Save Space for Vessel Cannulation When Treating Complex Aortic Aneurysms with Narrow Paravisceral Lumen Is Also Feasible Using Inner-Branched Pre-Cannulated Endografts
- PMID: 38892771
- PMCID: PMC11172520
- DOI: 10.3390/jcm13113060
Partial Deployment to Save Space for Vessel Cannulation When Treating Complex Aortic Aneurysms with Narrow Paravisceral Lumen Is Also Feasible Using Inner-Branched Pre-Cannulated Endografts
Abstract
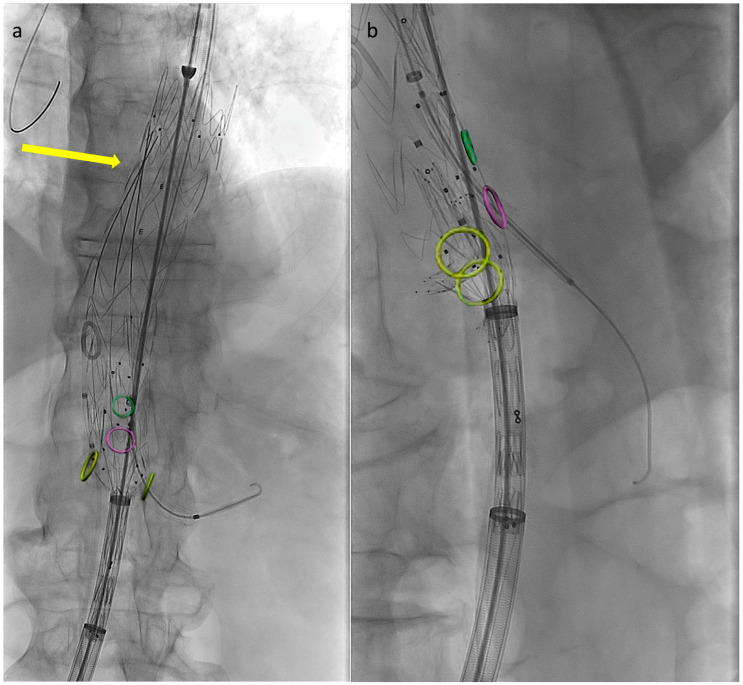
Introduction: The aim of this paper is to propose a sequential deployment technique for the E-nside off-the-shelf endograft that could potentially enhance target visceral vessel (TVV) cannulation and overstenting in narrow aortic anatomies. Methods: All data regarding patients consecutively treated in two aortic centers with the E-nside graft employing the partial deployment technique were included in the study cohort and analyzed. To execute the procedure with partial endograft deployment, the device should be prepared before insertion by advancing, under fluoroscopy, all four dedicated 400 cm long 0.018″ non-hydrophilic guidewires until their proximal ends reach the cranial graft's edge. Anticipating this guidewire placement prevents the inability to do so once the endograft is partially released, avoiding potentially increased friction inside the constricted pre-loaded microchannels. The endograft is then advanced and deployed in the standard fashion, stopping just after the inner branch outlets are fully expanded. Tip capture is released, and the proximal end of the device is opened. Visceral vessel bridging is completed from an upper access in the desired sequence, and the graft is fully released after revascularizing one or more arteries. Preventing the distal edge of the graft from fully expanding improves visceral vessel cannulation and bridging component advancement, especially when dealing with restricted lumina. Results: A total of 26 patients were treated during the period December 2019-March 2024 with the described approach. Procedure was performed in urgent settings in 14/26 cases. The available lumen was narrower than 24 mm at the origin of at least one target vessel in 11 out of 26 cases performed (42.3%). Technical success was obtained in 24 out of 26 cases (92.3%), with failures being due to TVVs loss. No intraoperative death or surgical conversion was recorded, and no early reintervention was needed in the perioperative period. Clinical success at 30 days was therefore 80.7%. Conclusions: The described technique could be considered effective in saving space outside of the graft, allowing for safe navigation and target vessel cannulation in narrow visceral aortas, similar to what has already been reported for outer-branched endografts.
Keywords: branched endograft; endovascular aortic repair; off-the-shelf endograft; thoracoabdominal aneurysm.
Conflict of interest statement
G.S., G.P. and GI are consultants for Artivion. The rest of the authors declare no conflict of interest.
Figures



References
-
- Oderich G.S., Forbes T.L., Chaer R., Davies M.G., Lindsay T.F., Mastracci T., Singh M.J., Timaran C., Woo E.Y. Writing Committee Group. Reporting standards for endovascular aortic repair of aneurysms involving the renal-mesenteric arteries. J. Vasc. Surg. 2021;73:4S–52S. doi: 10.1016/j.jvs.2020.06.011. - DOI - PubMed
-
- Abisi S., Zayed H., Frigatti P., Furlan F., Simonte G., Isernia G., Kuczmik W., Fattoum M., Halak M., Silverberg D., et al. Medium-term outcomes of EXTra-design engineering inner-branch ENdografts for the treatment of complex aortic aneurysms from a multicenter collaboration. J. Vasc. Surg. 2024 doi: 10.1016/j.jvs.2024.03.013. - DOI - PubMed
LinkOut - more resources
Full Text Sources
