

Videolaryngoscopy versus Fiberoptic Bronchoscopy for Awake Tracheal Intubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 38892899
- PMCID: PMC11173084
- DOI: 10.3390/jcm13113186
Videolaryngoscopy versus Fiberoptic Bronchoscopy for Awake Tracheal Intubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
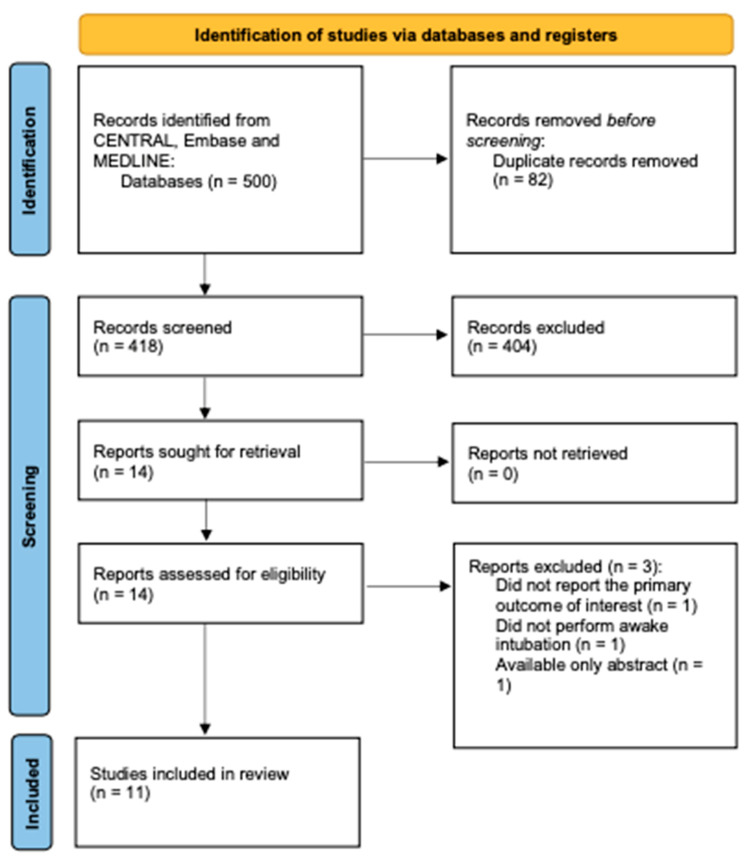
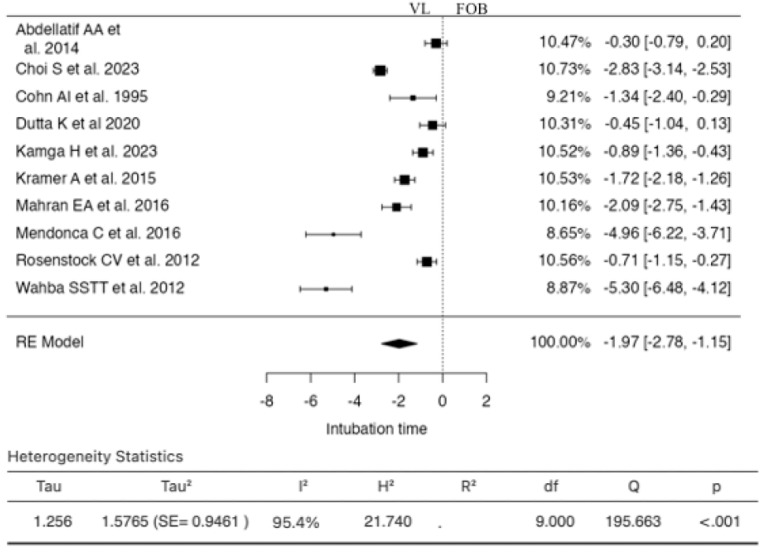
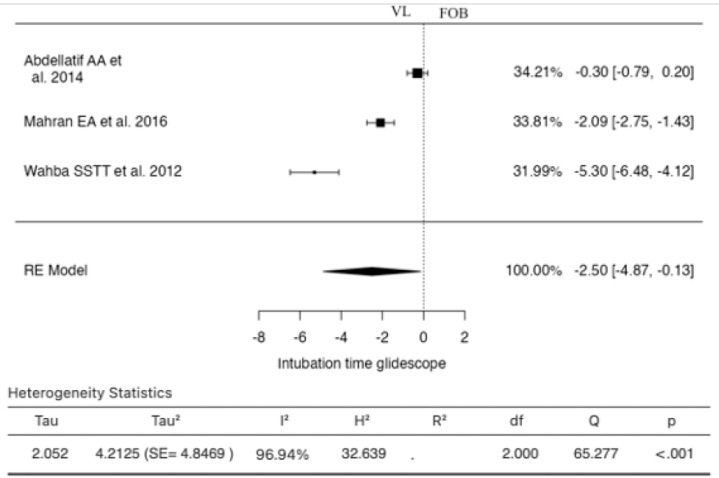
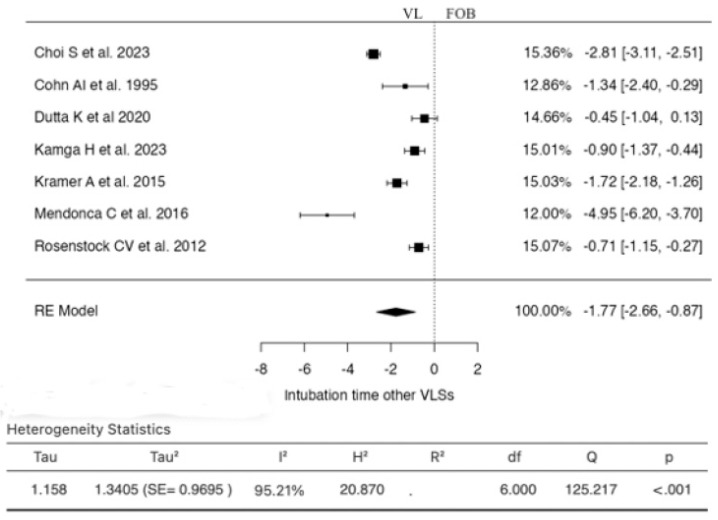
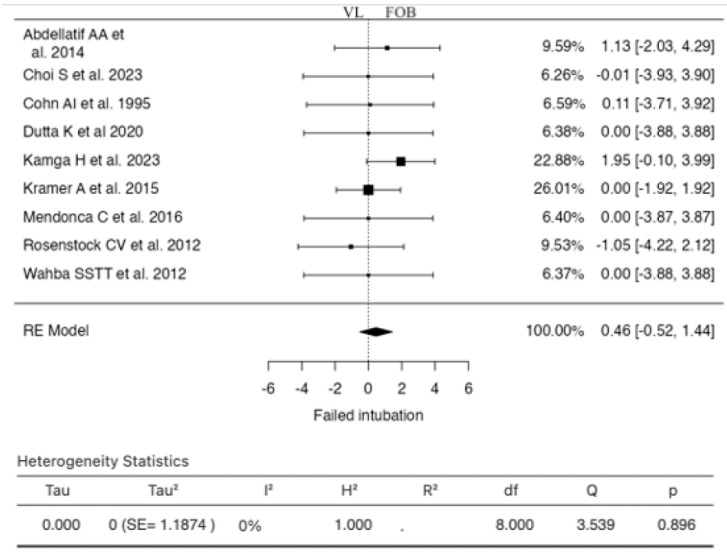
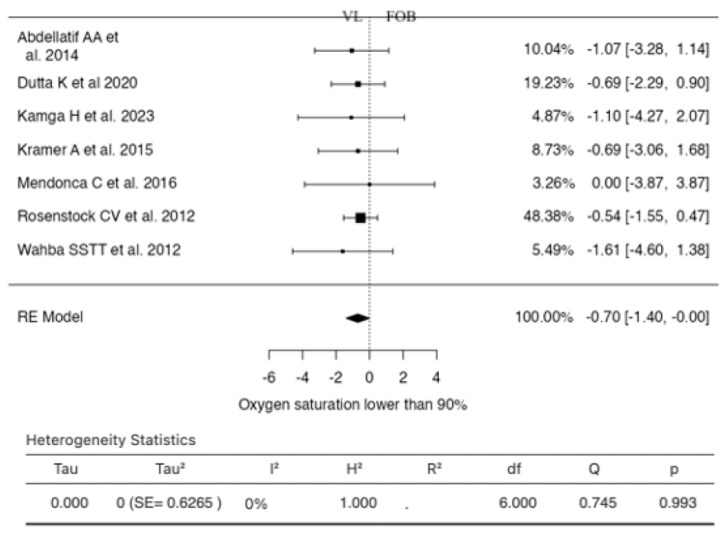
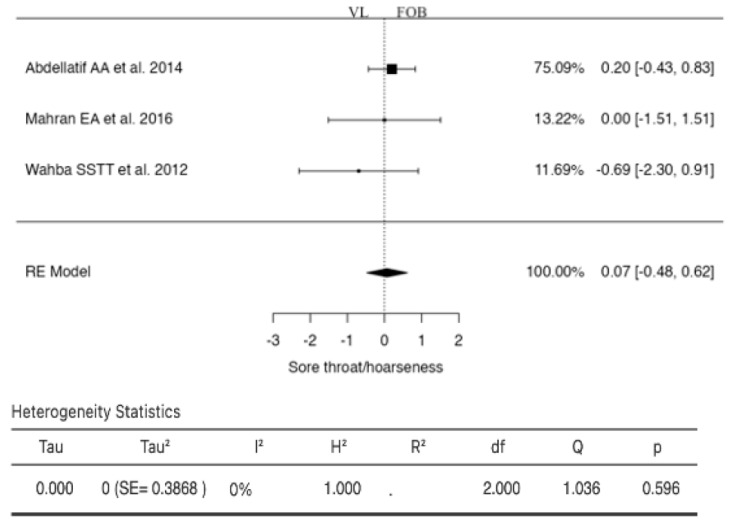
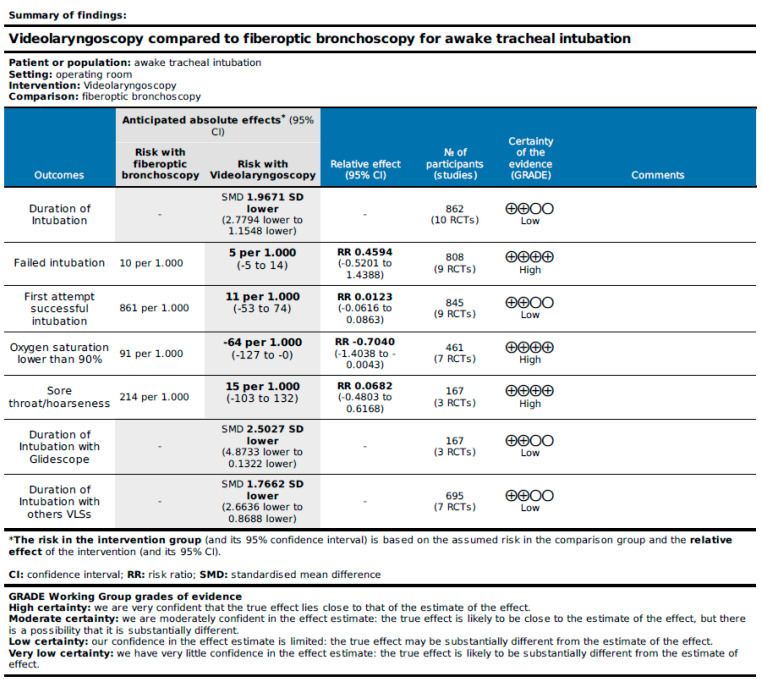
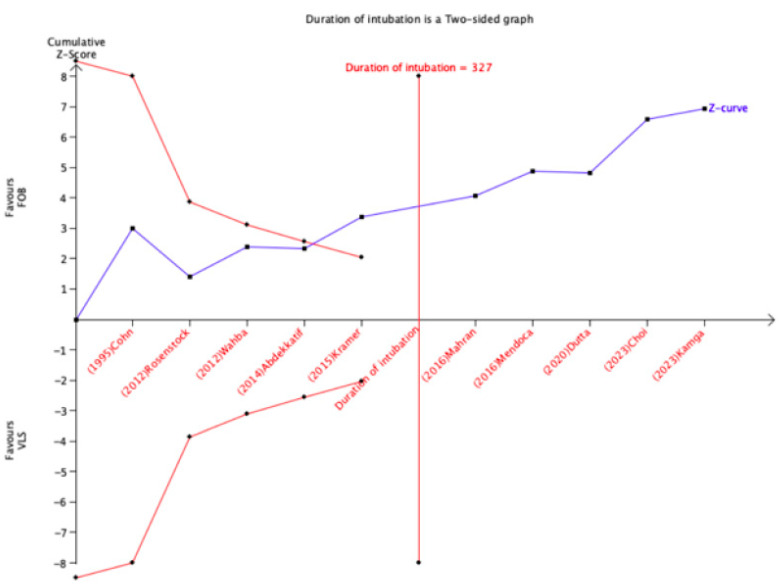
Background: In recent years, videolaryngoscopy has increasingly been utilized as an alternative to fiberoptic bronchoscopy in awake intubation. Nonetheless, it remains uncertain whether videolaryngoscopy represents a viable substitute for fiberoptic bronchoscopy. We conducted this systematic review with a meta-analysis to compare videolaryngoscopy and fiberoptic bronchoscopy for awake intubation. Methods: We systematically searched for all randomized controlled trials (RCTs) comparing videolaryngoscopy and fiberoptic bronchoscopy for awake intubation. The Cochrane Central Register of Controlled Trials (CENTRAL), Embase, and MEDLINE were systematically queried through August 2023. Our primary outcome measure was the duration of intubation. Secondary outcomes encompassed the rate of successful intubation on the initial attempt, failed intubation, patient-reported satisfaction, and any complications or adverse events potentially stemming from the intubation procedure. The Cochrane Risk of Bias Tool for RCTs was employed to evaluate all studies for evidence of bias. The GRADE approach was utilized to gauge the certainty of the evidence. Results: Eleven trials involving 873 patients were ultimately included in our review for data extraction. Meta-analysis demonstrated that videolaryngoscopy decreased the duration of intubation compared to fiberoptic bronchoscopy (SMD -1.9671 [95% CI: -2.7794 to -1.1548] p < 0.0001), a finding corroborated in subgroup analysis by the type of videolaryngoscope (SMD -2.5027 [95% CI: -4.8733 to -0.1322] p = 0.0385). Additionally, videolaryngoscopy marginally lowered the risk of experiencing a saturation below 90% during the procedure (RR -0.7040 [95% CI: -1.4038 to -0.0043] p = 0.0486). No statistically significant disparities were observed between the two techniques in terms of failed intubation, initial successful intubation attempt, or sore throat/hoarseness. With regard to patient-reported satisfaction, a pooled analysis was precluded due to the variability in evaluation methods employed across the trials to assess this outcome. Lastly, trial sequential analysis (TSA) conducted for intubation time (primary outcome) affirmed the conclusiveness of this evidence; TSA performed for secondary outcomes failed to yield conclusive evidence, indicating the necessity for further trials. Conclusions: Videolaryngoscopy for awake tracheal intubation diminishes intubation time and the risk of experiencing a saturation below 90% compared to fiberoptic bronchoscopy.
Keywords: airway management; awake intubation; fiberoptic bronchoscopy; meta-analysis; trial sequential analysis; videolaryngoscopy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Apfelbaum J.L., Hagberg C.A., Connis R.T., Abdelmalak B.B., Agarkar M., Dutton R.P., Fiadjoe J.E., Greif R., Klock P.A., Mercier D., et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022;136:31–81. doi: 10.1097/ALN.0000000000004002. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
