

Efficacy of Continuous Lumbar Plexus Blockade in Managing Post-Operative Pain after Hip or Femur Orthopedic Surgeries: A Systematic Review and Meta-Analysis
- PMID: 38892904
- PMCID: PMC11173339
- DOI: 10.3390/jcm13113194
Efficacy of Continuous Lumbar Plexus Blockade in Managing Post-Operative Pain after Hip or Femur Orthopedic Surgeries: A Systematic Review and Meta-Analysis
Abstract
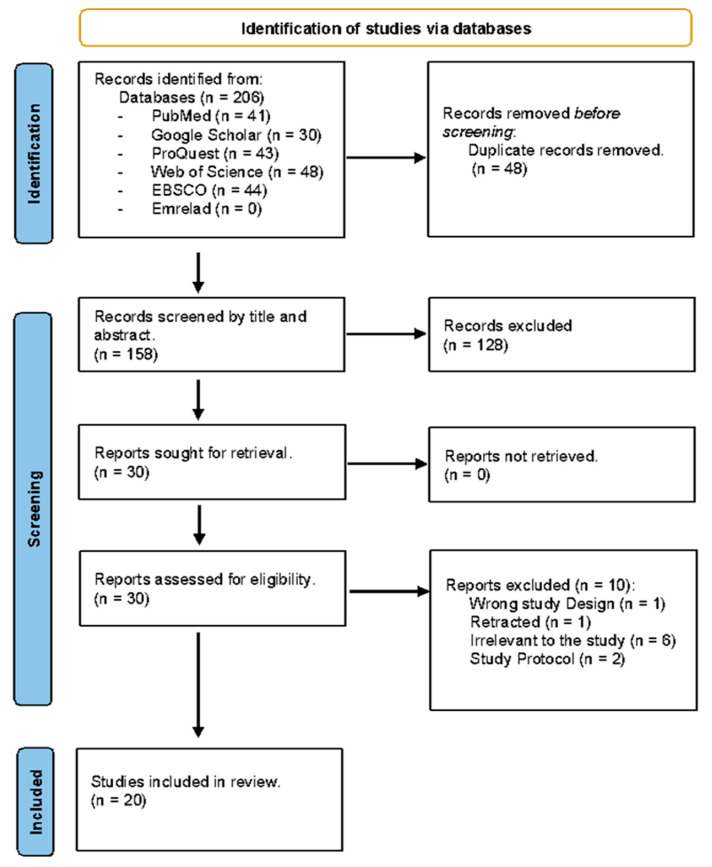
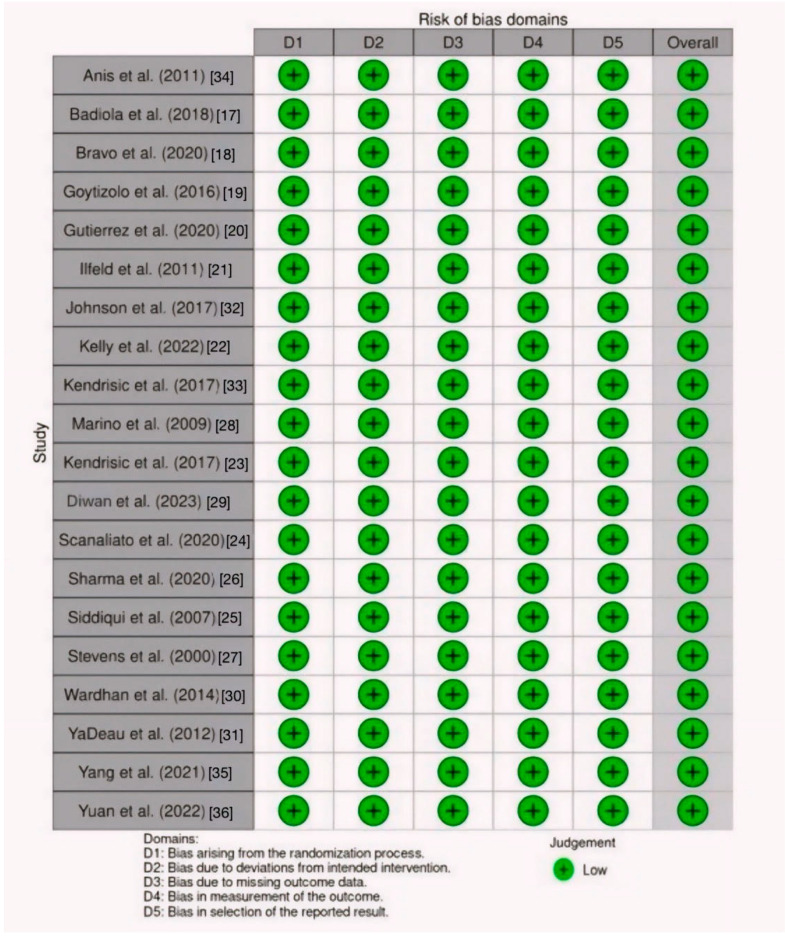
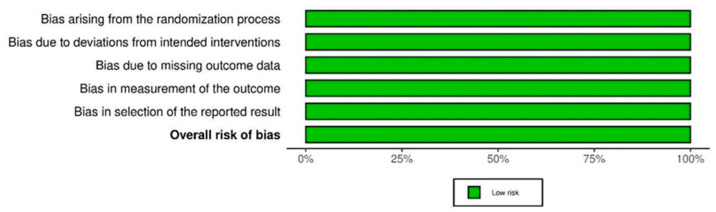
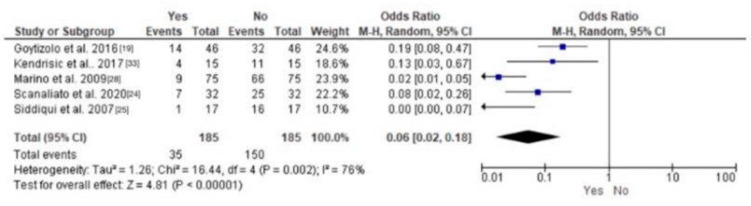
Background: Post-operative pain management is essential for optimizing recovery, patient comfort, and satisfaction. Peripheral nerve blockade, or lumbar plexus block (LPB), has been widely used for analgesia and regional anesthesia. This study explored the existing literature to determine the efficacy of continuous lumbar plexus blockade in managing post-operative pain following hip or femur surgery. Methods: Reviewers comprehensively searched electronic databases to identify peer-reviewed scholarly articles reporting the efficacy of lumbar plexus block in managing post-operative pain after orthopedic surgery. The potential articles were carefully selected and assessed for the risk of bias using the Cochrane Collaboration Risk of Bias assessment tool. Data were systematically extracted and analyzed. Results: The literature search yielded 206 articles, 20 of which were randomized controlled trials. Lumbar plexus block demonstrated superior pain relief compared to conventional pain management approaches like general anesthetics. In addition, LPB reduced patients' overall opioid consumption compared to controls, reduced adverse effects, and enhanced functional recovery, which underlines the broader positive impact of meticulous pain management. More patients could walk more than 40 feet after the second day post-operatively among the lumbar plexus group (14.7%) compared to the continuous femoral group (1.3%). Other parameters, including cortisol levels and hemodynamic stability, were evaluated, showing comparable outcomes. Conclusions: Lumbar plexus block is effective in pain management after orthopedic surgery, as shown by the lower pain scores and less opioid consumption. Additionally, patient satisfaction was relatively higher in LPB-treated patients compared to other approaches like general anesthesia.
Keywords: lumbar plexus block; orthopedic surgery; pain management.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






Similar articles
-
Continuous lumbar plexus block for postoperative pain control after total hip arthroplasty. A randomized controlled trial.J Bone Joint Surg Am. 2009 Jan;91(1):29-37. doi: 10.2106/JBJS.H.00079. J Bone Joint Surg Am. 2009. PMID: 19122076 Clinical Trial.
-
Continuous lumbar plexus block provides improved analgesia with fewer side effects compared with systemic opioids after hip arthroplasty: a randomized controlled trial.Reg Anesth Pain Med. 2007 Sep-Oct;32(5):393-8. doi: 10.1016/j.rapm.2007.04.008. Reg Anesth Pain Med. 2007. PMID: 17961837 Clinical Trial.
-
Lumbar plexus block reduces pain and blood loss associated with total hip arthroplasty.Anesthesiology. 2000 Jul;93(1):115-21. doi: 10.1097/00000542-200007000-00021. Anesthesiology. 2000. PMID: 10861154 Clinical Trial.
-
Pain Management After Hip Arthroscopy: Systematic Review of Randomized Controlled Trials and Cohort Studies.Am J Sports Med. 2018 Nov;46(13):3288-3298. doi: 10.1177/0363546517734518. Epub 2017 Oct 13. Am J Sports Med. 2018. PMID: 29028436
-
Efficacy and adverse effects of peripheral nerve blocks and local infiltration anesthesia after arthroscopic shoulder surgery: A Bayesian network meta-analysis.Front Med (Lausanne). 2022 Nov 10;9:1032253. doi: 10.3389/fmed.2022.1032253. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36438028 Free PMC article.
Cited by
-
From Pain Control to Early Mobility: The Evolution of Regional Anesthesia in Geriatric Total Hip Arthroplasty.Reports (MDPI). 2025 May 9;8(2):64. doi: 10.3390/reports8020064. Reports (MDPI). 2025. PMID: 40710855 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
