

Croco Eye Technique: Mucous Retention Cyst Excision with Immediate Open Sinus Lift-A Retrospective Cohort Study
- PMID: 38893004
- PMCID: PMC11172874
- DOI: 10.3390/jcm13113293
Croco Eye Technique: Mucous Retention Cyst Excision with Immediate Open Sinus Lift-A Retrospective Cohort Study
Abstract
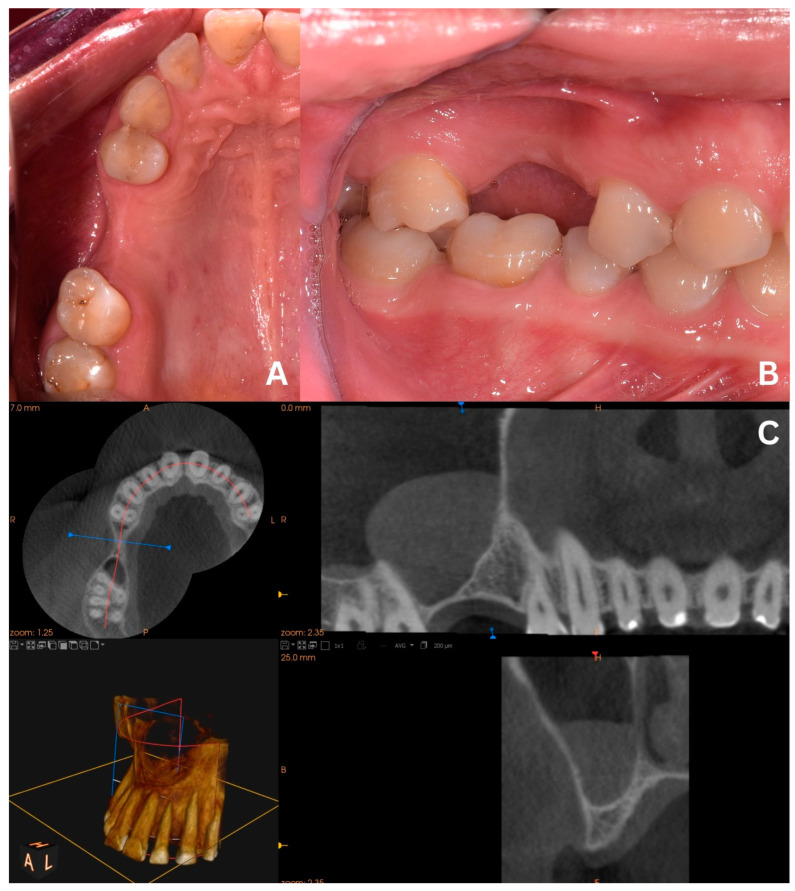
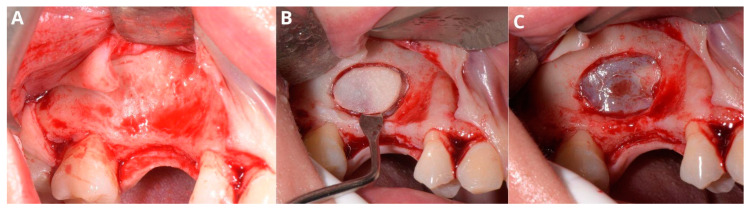
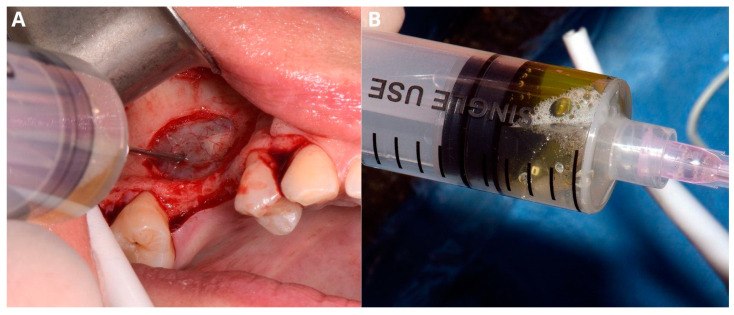
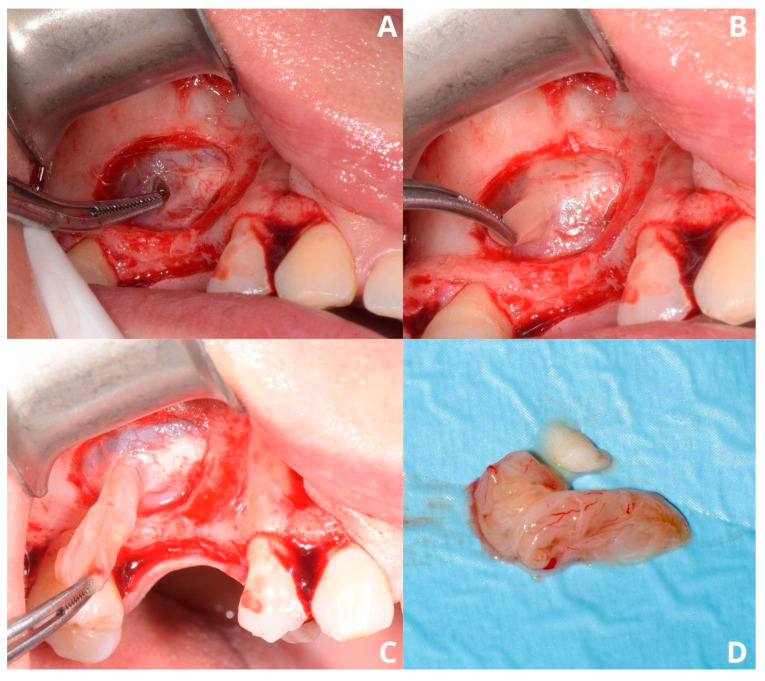
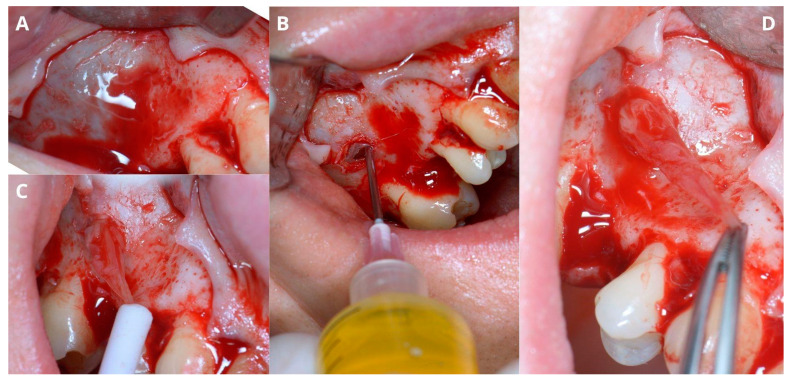
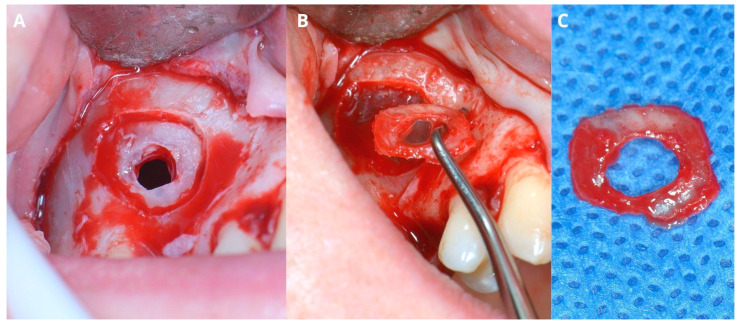
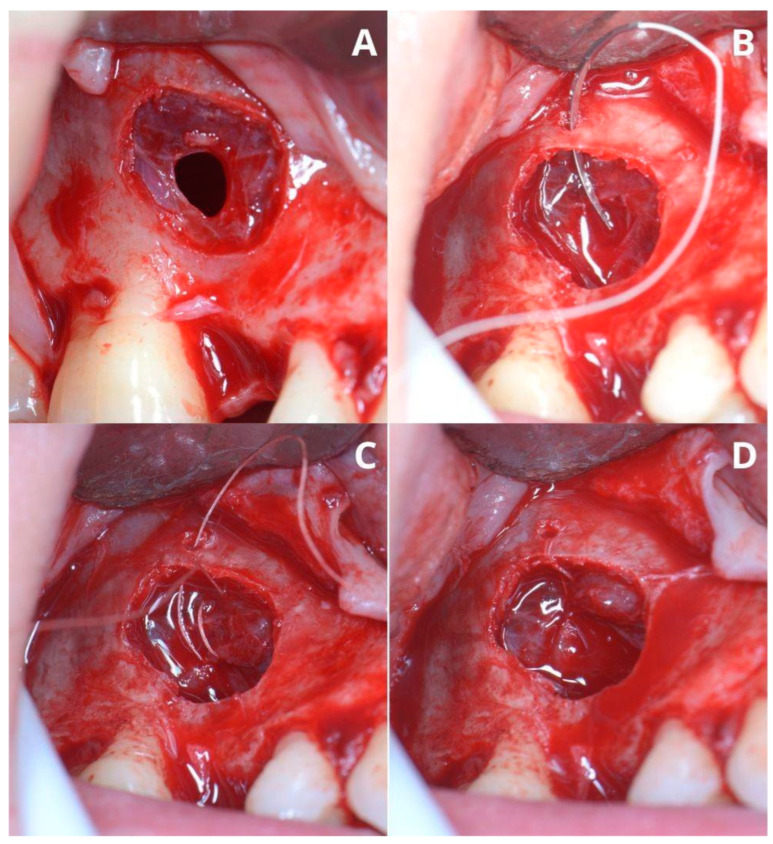
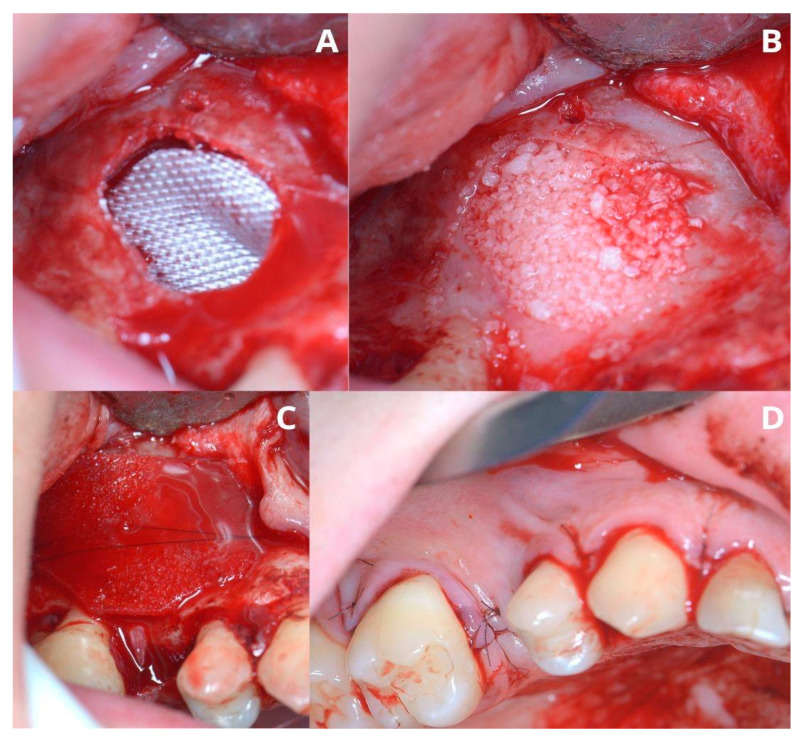
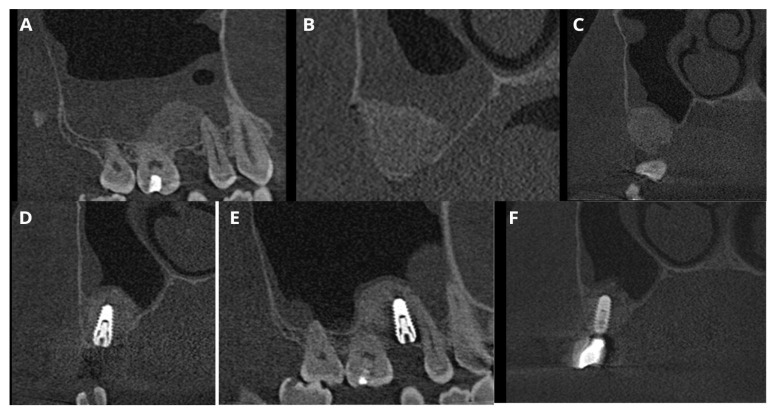
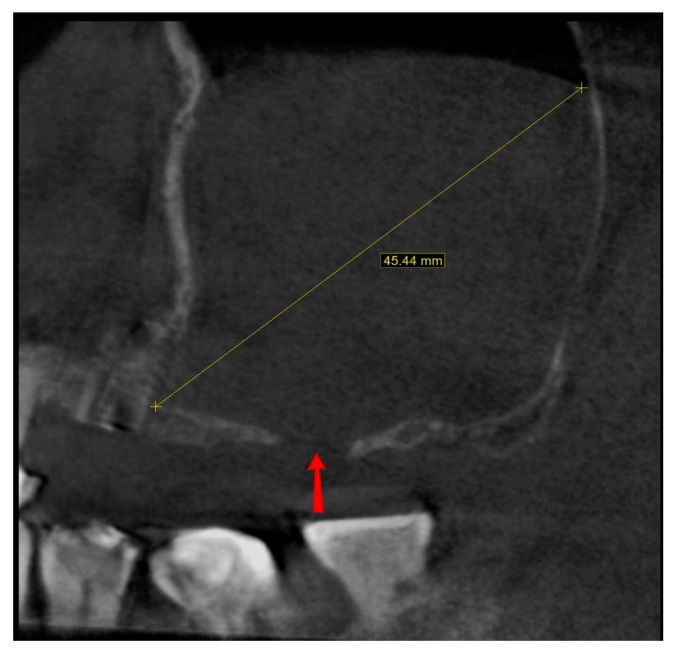
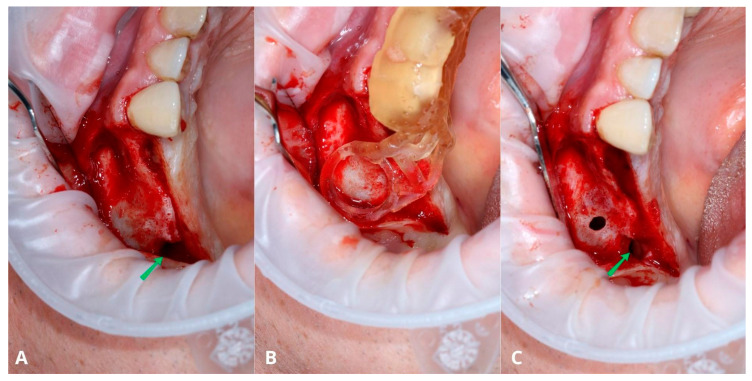
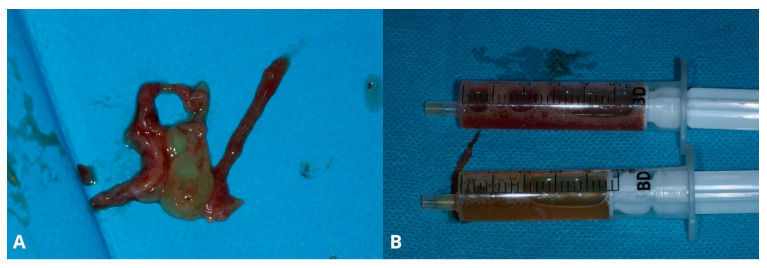
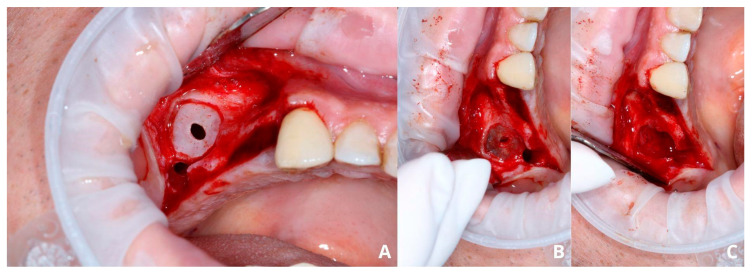
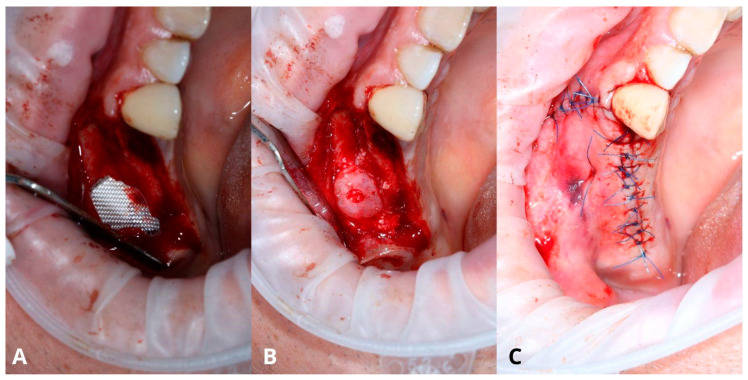
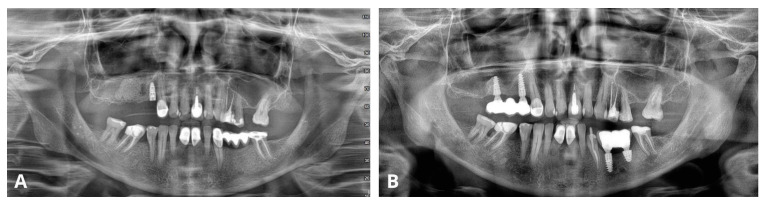
Objectives: A mucous retention cyst is a common, asymptomatic lesion that may cause complications during or after the sinus lift procedure. The goal of this study is to assess the effectiveness of the Croco Eye Technique (CET), which allows simultaneous excision of the cyst and sinus floor elevation. Methods: The technique was thoroughly described in two versions, and the group of 33 patients was analyzed. Patients who qualified for this procedure had insufficient alveolar ridge height, and their CBCT showed radiological images typical for retention cysts. Analyzed parameters included the version of CET, demographic data, anatomical parameters, intraoperative complications, recurrence of the cyst, success rate of the sinus lift and implants, and the follow-up period. Results: Out of the 33 cases, 9 were of the primary version (27.27%) and 24 of the final version (72.73%). The average height of a retention cyst was 24.05 mm, with the average alveolar ridge height of 1.86 mm. In three cases (9.09%), implants were placed immediately. The prevalence of uncontrolled Schneiderian membrane perforation was reduced from 55.56% to 4.17% between the primary and final versions. The cyst's recurrence rate was 3.13%. The implant survival rate was 100%. The mean follow-up period was 48.625 months (max 110 months). Conclusions: The Croco Eye Technique, despite the perforation of the Schneiderian membrane, enables successful sinus lift and implantation with a success rate of 100%. Excision of the retention cyst, which is the cause of perforation, allows for limiting the risk of the cyst's recurrence.
Keywords: biopsy; croco eye technique; excision; mucous retention cyst; retrospective cohort study; sinus floor elevation; sinus lift.
Conflict of interest statement
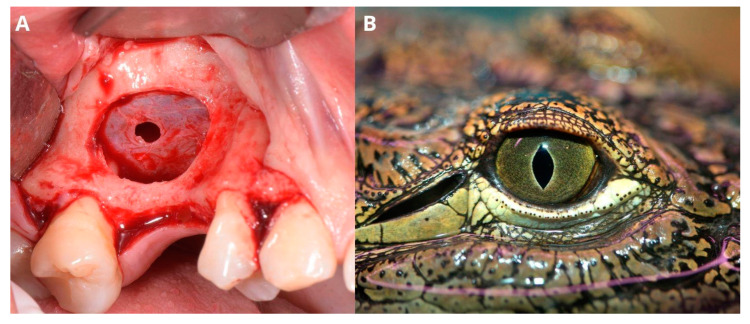
The authors declare no conflicts of interest. The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. The photography of a crocodile eye (Figure 5B) was purchased via Canva Pro (Canva Pty Ltd., Perth, Australia).
Figures
Similar articles
-
Radiological sinus lift: a new minimally invasive CT-guided procedure for maxillary sinus floor elevation in implant dentistry.Clin Oral Implants Res. 2016 Mar;27(3):341-7. doi: 10.1111/clr.12549. Epub 2015 Jan 13. Clin Oral Implants Res. 2016. PMID: 25583141
-
Lateral approach for maxillary sinus membrane elevation without bone materials in maxillary mucous retention cyst with immediate or delayed implant rehabilitation: case reports.J Korean Assoc Oral Maxillofac Surg. 2017 Aug;43(4):276-281. doi: 10.5125/jkaoms.2017.43.4.276. Epub 2017 Aug 24. J Korean Assoc Oral Maxillofac Surg. 2017. PMID: 28875144 Free PMC article.
-
[Elimination of defects in the Schneiderian membrane during sinus lift operations].Stomatologiia (Mosk). 2024;103(1):31-34. doi: 10.17116/stomat202410301131. Stomatologiia (Mosk). 2024. PMID: 38372604 Russian.
-
Are mucous retention cysts and pseudocysts in the maxillary sinus a risk factor for dental implants? A systematic review.Med Oral Patol Oral Cir Bucal. 2021 May 1;26(3):e276-e283. doi: 10.4317/medoral.24155. Med Oral Patol Oral Cir Bucal. 2021. PMID: 33247569 Free PMC article.
-
Influence of exposing dental implants into the sinus cavity on survival and complications rate: a systematic review.Int J Implant Dent. 2019 Feb 5;5(1):6. doi: 10.1186/s40729-019-0157-7. Int J Implant Dent. 2019. PMID: 30719578 Free PMC article. Review.
Cited by
-
One-Stage Surgical Management of an Asymptomatic Maxillary Sinus Mucocele with Immediate Lateral Sinus Lift and Simultaneous Implant Placement: A Case Report.J Clin Med. 2025 Mar 13;14(6):1946. doi: 10.3390/jcm14061946. J Clin Med. 2025. PMID: 40142753 Free PMC article.
References
LinkOut - more resources
Full Text Sources
