

All-on-4 Hybrid with Extra-Long Transnasal Implants: Descriptions of the Technique and Short-Term Outcomes in Three Cases
- PMID: 38893060
- PMCID: PMC11172536
- DOI: 10.3390/jcm13113348
All-on-4 Hybrid with Extra-Long Transnasal Implants: Descriptions of the Technique and Short-Term Outcomes in Three Cases
Abstract
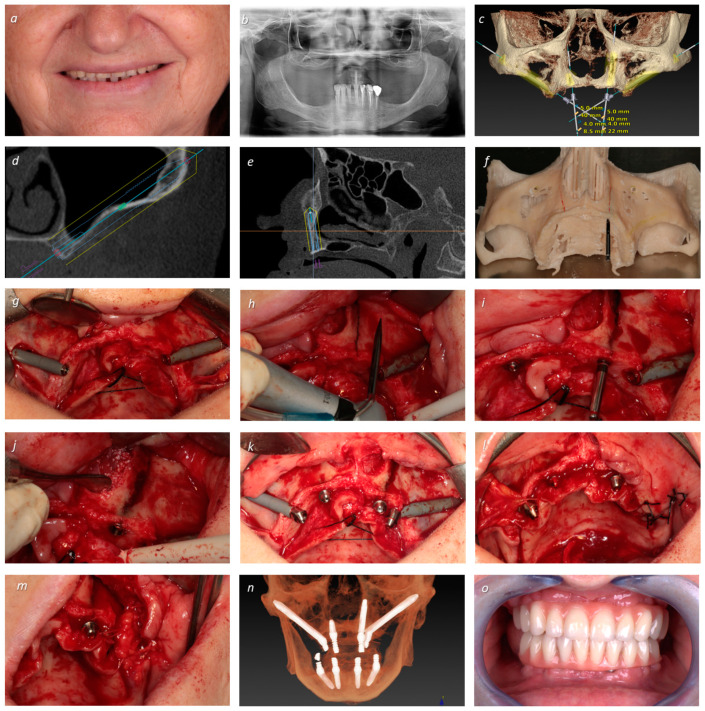
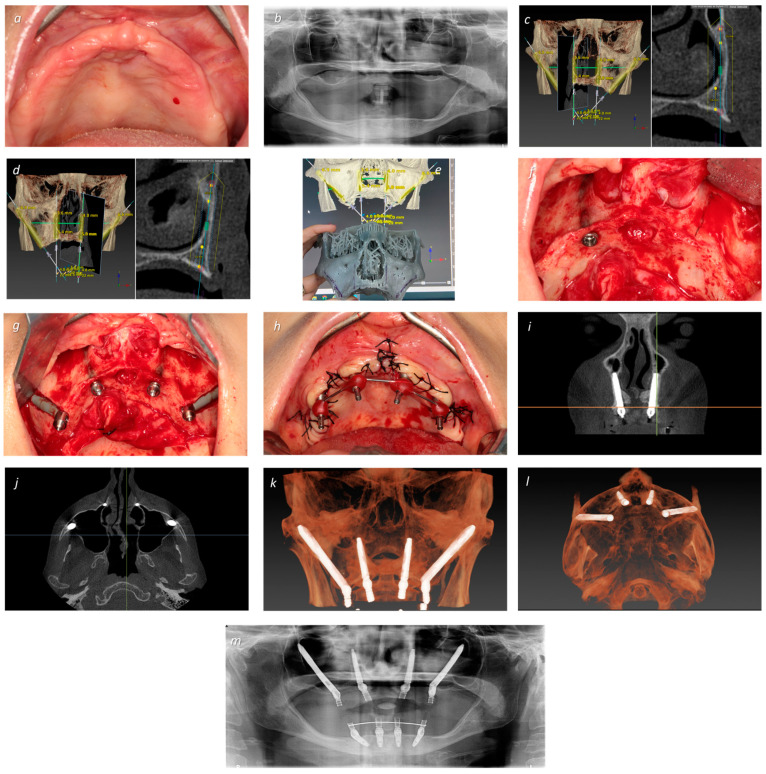
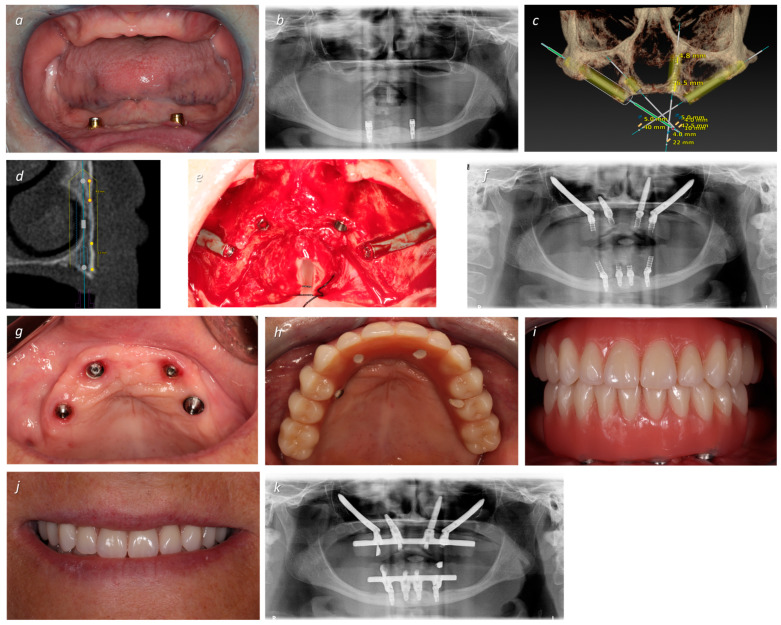
Background/Objectives: There is a need for alternative approaches to full-arch rehabilitation of atrophic maxillae. The aim of this short case series was to describe the technique and assess the short term-outcomes of atrophic maxillae rehabilitation using transnasal implants in conjunction with zygomatic implants. Methods: Three female patients (average age: 62 years) presenting comorbidities and atrophic maxillae preventing the insertion of standard maxillary anchored implants received a full-arch fixed prosthesis supported by transnasal implants together with zygomatic implants, using the ad modum all-on-4 concept. Patients were followed during the functional osseointegration period. Primary outcome measures were prosthetic and implant survival based on function. Secondary outcome measures were complication parameters (biological and mechanical), plaque and bleeding levels, and probing pocket depths > 4 mm. Results: No implant failures were registered, and all prostheses remained in function. The only complication was a fracture of a provisional crown that was resolved. Plaque and bleeding scores were mild during the follow-up period. Conclusions: The present manuscript describes the use of extra-long transnasal implants in combination with zygomatic implants in immediate function for full-arch fixed prosthetic rehabilitation of atrophic maxillae, with the objective of promoting more research into this relatively recent technique. More studies are needed to validate the technique.
Keywords: all-on-4; dental implants; transnasal; zygomatic implants.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Five-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded zygomatic implants placed extra-maxillary.Eur J Oral Implantol. 2014 Autumn;7(3):267-81. Eur J Oral Implantol. 2014. PMID: 25237671
-
Immediate full-arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: a prospective clinical study with minimum follow-up of 6 years.Int J Oral Maxillofac Surg. 2017 Dec;46(12):1592-1599. doi: 10.1016/j.ijom.2017.05.023. Epub 2017 Jun 24. Int J Oral Maxillofac Surg. 2017. PMID: 28655434
-
Zygomatic Implants Placed in Immediate Function through Extra-Maxillary Surgical Technique and 45 to 60 Degrees Angulated Abutments for Full-Arch Rehabilitation of Extremely Atrophic Maxillae: Short-Term Outcome of a Retrospective Cohort.J Clin Med. 2021 Aug 16;10(16):3600. doi: 10.3390/jcm10163600. J Clin Med. 2021. PMID: 34441896 Free PMC article.
-
Rehabilitation of the severely resorbed maxilla by using quad zygomatic implant-supported prostheses: a systematic review and meta-analysis.J Prosthet Dent. 2023 Oct;130(4):543-552. doi: 10.1016/j.prosdent.2021.11.007. Epub 2021 Dec 14. J Prosthet Dent. 2023. PMID: 34920870 Review.
-
The Moderately Atrophic Maxilla: Trans-Sinus/Transnasal Approaches.Atlas Oral Maxillofac Surg Clin North Am. 2025 Sep;33(2):129-139. doi: 10.1016/j.cxom.2025.06.002. Atlas Oral Maxillofac Surg Clin North Am. 2025. PMID: 40818861 Review. No abstract available.
References
-
- World Health Organization . World Health Organization; 2023. [(accessed on 24 March 2024)]. Oral Health. Available online: https://www.who.int/health-topics/oral-health#tab=tab_1.
LinkOut - more resources
Full Text Sources
Medical
