

Reasons for Discordance between 68Ga-PSMA-PET and Magnetic Resonance Imaging in Men with Metastatic Prostate Cancer
- PMID: 38893178
- PMCID: PMC11171071
- DOI: 10.3390/cancers16112056
Reasons for Discordance between 68Ga-PSMA-PET and Magnetic Resonance Imaging in Men with Metastatic Prostate Cancer
Abstract
Background: PSMA PET has emerged as a "gold standard" imaging modality for assessing prostate cancer metastases. However, it is not universally available, and this limits its impact. In contrast, whole-body MRI is much more widely available but misses more lesions. This study aims to improve the interpretation of whole-body MRI by comparing false negative scans retrospectively to PSMA PET.
Methods: This study was a retrospective sub-analysis of a prospectively collected database of patients who participated in a clinical trial of PSMA PET/MRI comparing PSMA PET and whole-body MRI from 2018-2021. Subjects whose separately read PSMA PET and MRI diagnostic reports showed discrepancies ("false negative" MRI cases) were selected for sub-analysis. The cases were reviewed by the same attending radiologist who originally read the scans. The radiologist noted specific features on MRI indicating metastatic disease that were initially missed.
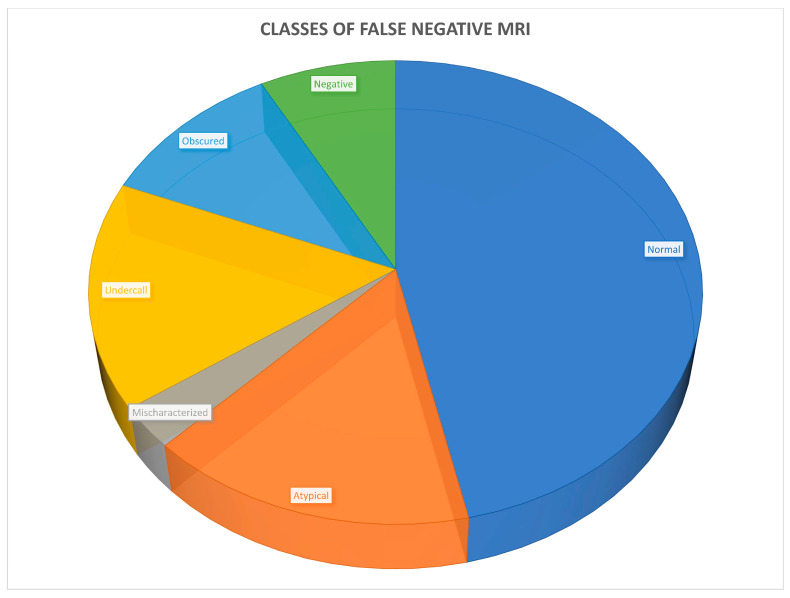
Results: Of 263 cases, 38 (14%) met the inclusion criteria and were reviewed. Six classes of mpMRI false negatives were identified: anatomically normal (18, 47%), atypical MRI appearance (6, 16%), mischaracterization (1, 3%), undercall (6, 16%), obscured (4, 11%), and no abnormality on MRI (3, 8%). Considering that the atypical and undercalled cases could have been adjusted in retrospect, and that 4 additional cases had positive lesions to the same extent and 11 further cases had disease confined to the pelvis, only 11 (4%) of the original 263 would have had disease outside of a conventional radiation treatment plan.
Conclusion: Notably, almost 50% of the cases, including most lymph node metastases, were anatomically normal using standard criteria. This suggests that current anatomic criteria for evaluating prostate cancer lymph node metastases are not ideal, and there is a need for improved criteria. In addition, 32% of cases involved some element of human interpretive error, and, therefore, improving reader training may lead to more accurate results.
Keywords: MRI; PET; PSMA; cancer; prostate; whole-body.
Conflict of interest statement
John Babich is Founder, President and Chief Scientific Officer, Ratio Therapeutics, Inc. Daniel J. A. Margolis has received an ad hoc consulting consideration from Guerbet and Promaxo. None of these companies was involved in the funding or analysis of the data herein. The Corresponding Author assumes ultimate responsibility for the content.
Figures




Similar articles
-
Positron emission tomography (PET) and magnetic resonance imaging (MRI) for the assessment of axillary lymph node metastases in early breast cancer: systematic review and economic evaluation.Health Technol Assess. 2011 Jan;15(4):iii-iv, 1-134. doi: 10.3310/hta15040. Health Technol Assess. 2011. PMID: 21276372 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2013 Apr;17(16):1-243. doi: 10.3310/hta17160. Health Technol Assess. 2013. PMID: 23611316 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Intraoperative frozen section analysis for the diagnosis of early stage ovarian cancer in suspicious pelvic masses.Cochrane Database Syst Rev. 2016 Mar 1;3(3):CD010360. doi: 10.1002/14651858.CD010360.pub2. Cochrane Database Syst Rev. 2016. PMID: 26930463 Free PMC article.
References
-
- American Society of Clinical Oncology Prostate Cancer Statistics. [(accessed on 25 September 2021)]. Available online: https://www.cancer.net/cancer-types/prostate-cancer/statistics.
-
- Zumsteg Z.S., Spratt D.E., Romesser P.B., Pei X., Zhang Z., Polkinghorn W., McBride S., Kollmeier M., Yamada Y., Zelefsky M.J. The natural history and predictors of outcome following biochemical relapse in the dose escalation era for prostate cancer patients undergoing definitive external beam radiotherapy. Eur. Urol. 2015;67:1009–1016. doi: 10.1016/j.eururo.2014.09.028. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
