

Disease Control and Toxicity Outcomes after Stereotactic Ablative Radiation Therapy for Recurrent and/or Metastatic Cancers in Young-Adult and Pediatric Patients
- PMID: 38893209
- PMCID: PMC11171376
- DOI: 10.3390/cancers16112090
Disease Control and Toxicity Outcomes after Stereotactic Ablative Radiation Therapy for Recurrent and/or Metastatic Cancers in Young-Adult and Pediatric Patients
Abstract
Background: Pediatric patients with metastatic and/or recurrent solid tumors have poor survival outcomes despite standard-of-care systemic therapy. Stereotactic ablative radiation therapy (SABR) may improve tumor control. We report the outcomes with the use of SABR in our pediatric solid tumor population.
Methods: This was a single-institutional study in patients < 30 years treated with SABR. The primary endpoint was local control (LC), while the secondary endpoints were progression-free survival (PFS), overall survival (OS), and toxicity. The survival analysis was performed using Kaplan-Meier estimates in R v4.2.3.
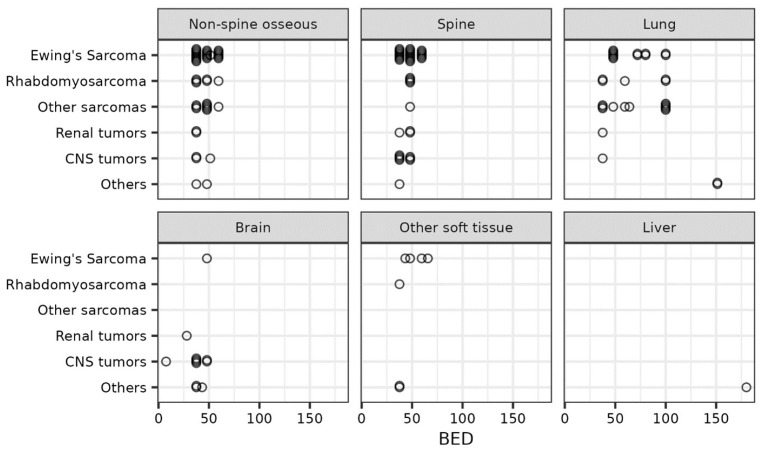
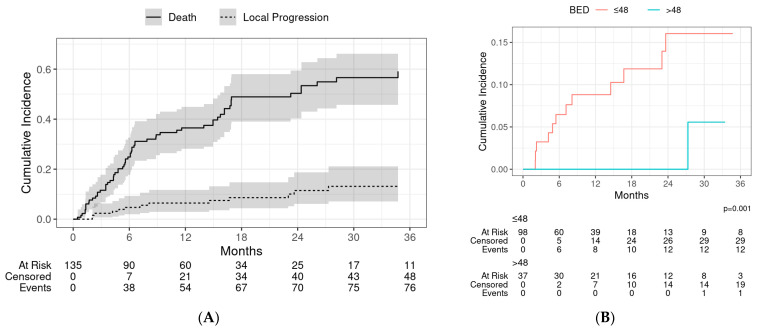
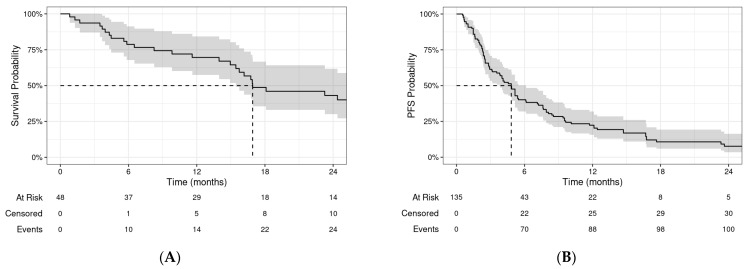
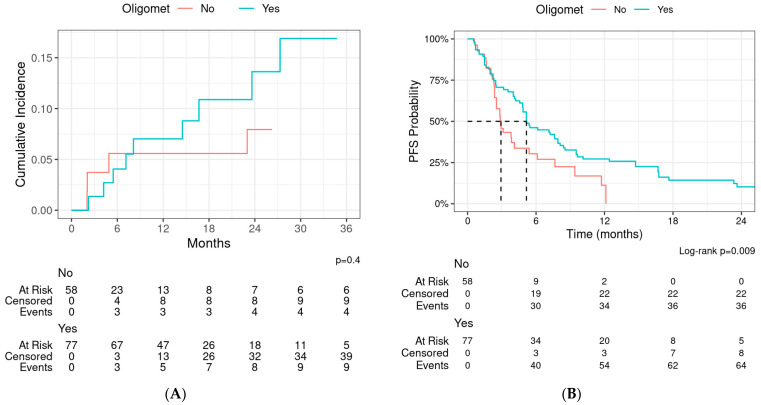
Results: In total, 48 patients receiving 135 SABR courses were included. The median age was 15.6 years (interquartile range, IQR 14-23 y) and the median follow-up was 18.1 months (IQR: 7.7-29.1). The median SABR dose was 30 Gy (IQR 25-35 Gy). The most common primary histologies were Ewing sarcoma (25%), rhabdomyosarcoma (17%), osteosarcoma (13%), and central nervous system (CNS) gliomas (13%). Furthermore, 57% of patients had oligometastatic disease (≤5 lesions) at the time of SABR. The one-year LC, PFS, and OS rates were 94%, 22%, and 70%, respectively. No grade 4 or higher toxicities were observed, while the rates of any grade 1, 2, and 3 toxicities were 11.8%, 3.7%, and 4.4%, respectively. Patients with oligometastatic disease, lung, or brain metastases and those who underwent surgery for a metastatic site had a significantly longer PFS. LC at 1-year was significantly higher for patients with a sarcoma histology (95.7% vs. 86.5%, p = 0.01) and for those who received a biological equivalent dose (BED10) > 48 Gy (100% vs. 91.2%, p = 0.001).
Conclusions: SABR is well tolerated in pediatric patients with 1-year local failure and OS rates of <10% and 70%, respectively. Future studies evaluating SABR in combination with systemic therapy are needed to address progression outside of the irradiated field.
Keywords: SABR; metastatic cancer; pediatric cancer; stereotactic body radiotherapy; systemic therapy.
Conflict of interest statement
J.D.P. reports serving on the Novocure Advisory Board and receiving consulting fees from More Health and Huron consultant and grant funding from Varian Medical Systems, Genentech, and NIH R702 and NIH R01 outside the submitted work. None of the other authors have relevant conflicts of interest.
Figures
References
-
- Kager L., Zoubek A., Pötschger U., Kastner U., Flege S., Kempf-Bielack B., Branscheid D., Kotz R., Salzer-Kuntschik M., Winkelmann W., et al. Primary Metastatic Osteosarcoma: Presentation and Outcome of Patients Treated on Neoadjuvant Cooperative Osteosarcoma Study Group Protocols. J. Clin. Oncol. 2003;21:2011–2018. doi: 10.1200/JCO.2003.08.132. - DOI - PubMed
-
- Mertens A.C., Yasui Y., Neglia J.P., Potter J.D., Nesbit M.E., Ruccione K., Smithson W.A., Robison L.L. Late Mortality Experience in Five-Year Survivors of Childhood and Adolescent Cancer: The Childhood Cancer Survivor Study. J. Clin. Oncol. 2001;19:3163–3172. doi: 10.1200/JCO.2001.19.13.3163. - DOI - PubMed
LinkOut - more resources
Full Text Sources
