

Uterine Arteriovenous Malformation: Diagnostic and Therapeutic Challenges
- PMID: 38893611
- PMCID: PMC11172076
- DOI: 10.3390/diagnostics14111084
Uterine Arteriovenous Malformation: Diagnostic and Therapeutic Challenges
Abstract
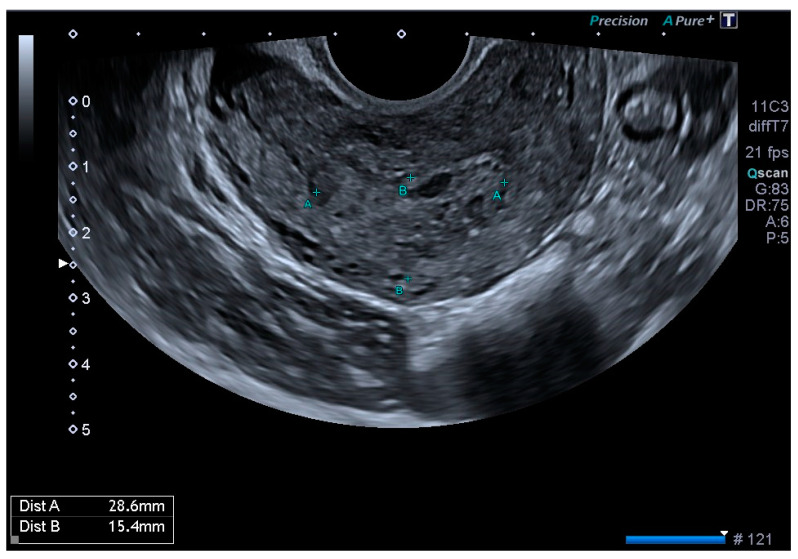
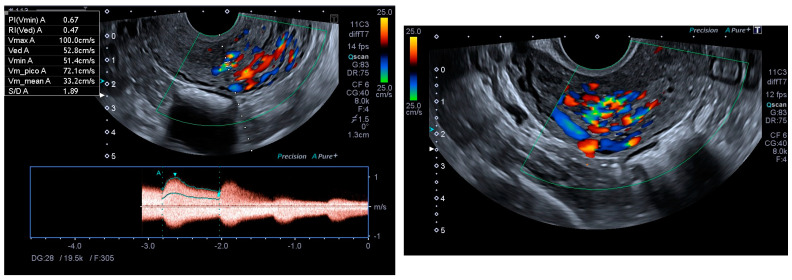
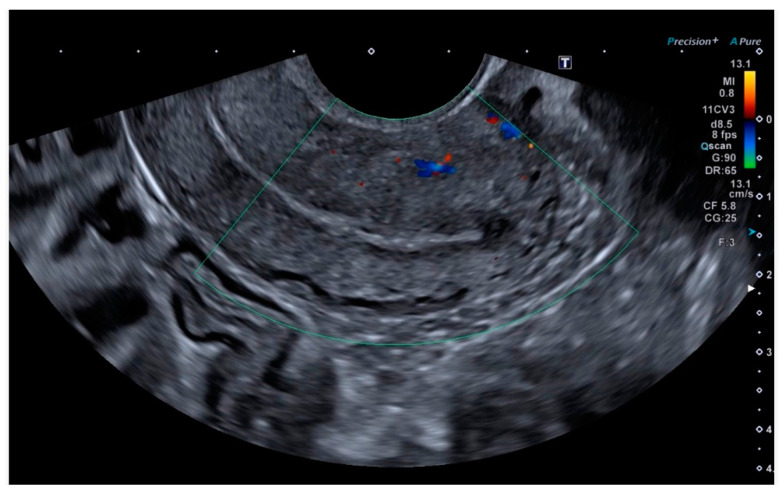
Uterine arteriovenous malformations are a rare cause of puerperal haemorrhage, but their incidence is increasing due to both improved diagnosis and the more frequent use of uterine surgery in recent years. The use of ultrasound, both B-mode and Doppler, is recommended for diagnosis and follow-up, as it has been shown to be the simplest and most cost-effective method. Endometrial thickening associated with an anechoic and vascular intramiometrial structure is very useful for diagnosis and can help to exclude other causes of dysfunctional bleeding. Pulsed Doppler shows low-resistance vessels and high pulsatility indices with a high peak systolic velocity (PSV). In a healthy myometrium, the vessels have a peak systolic velocity of 9-40 cm/s and a resistance index between 0.6 and 0.8, whereas in the case of AVMs, the systolic and diastolic velocities are 4-6 times higher (PSV 25-110 cm/s with a mean of 60 cm/s and a resistance index of 0.27-0.75 with a mean of 0.41). For treatment, we must individualise each case, taking into account haemodynamic stability, the patient's reproductive wishes, and the severity of the AVM as assessed by its size and PSV.
Keywords: Doppler ultrasound; myometrial hypervascularisation; peak systolic velocity; uterine arteriovenous malformation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Ultrasound diagnosis and management of acquired uterine enhanced myometrial vascularity/arteriovenous malformations.Am J Obstet Gynecol. 2016 Jun;214(6):731.e1-731.e10. doi: 10.1016/j.ajog.2015.12.024. Epub 2016 Feb 9. Am J Obstet Gynecol. 2016. PMID: 26873276
-
Use of hysteroscopy in diagnosis and follow-up of acquired uterine enhanced myometrial vascularity.Fertil Steril. 2020 Feb;113(2):460-462. doi: 10.1016/j.fertnstert.2019.11.006. Fertil Steril. 2020. PMID: 32106997
-
Ultrasonographic technique to differentiate enhanced myometrial vascularity/arteriovenous malformation from retained products of conception.J Ultrasound. 2022 Jun;25(2):379-386. doi: 10.1007/s40477-021-00574-y. Epub 2021 Mar 2. J Ultrasound. 2022. PMID: 33651329 Free PMC article.
-
Treatment of uterine arteriovenous malformation by myometrial lesion resection combined with artery occlusion under laparoscopy: a case report and literature review.Eur J Obstet Gynecol Reprod Biol. 2013 Jul;169(2):172-6. doi: 10.1016/j.ejogrb.2013.04.009. Epub 2013 May 31. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 23727224 Review.
-
Color Doppler US in the evaluation of uterine vascular abnormalities.Radiographics. 2002 Jan-Feb;22(1):47-53. doi: 10.1148/radiographics.22.1.g02ja0947. Radiographics. 2002. PMID: 11796897 Review.
Cited by
-
An unsuspected case of uterine arteriovenous malformation with nidus aneurysm following vaginal delivery: Diagnostic challenges and management.Radiol Case Rep. 2025 Mar 11;20(5):2624-2630. doi: 10.1016/j.radcr.2025.01.006. eCollection 2025 May. Radiol Case Rep. 2025. PMID: 40129827 Free PMC article.
-
Selective Conventional Approach for Management of Bleeding Uterine Arteriovenous Malformation: A Case Report.JNMA J Nepal Med Assoc. 2025 Feb;63(282):120-122. doi: 10.31729/jnma.8891. Epub 2025 Feb 28. JNMA J Nepal Med Assoc. 2025. PMID: 40656829 Free PMC article.
References
-
- Gan F., Vikneswaran V., Yu K.K. Uterine arteriovenous malformation. Possible association to uterine fibroids? Med. J. Malaysia. 2021;76:273–274. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
