

Ultrasound-Assisted and Ultrasound-Guided Thoracentesis: An Educational Review
- PMID: 38893651
- PMCID: PMC11172328
- DOI: 10.3390/diagnostics14111124
Ultrasound-Assisted and Ultrasound-Guided Thoracentesis: An Educational Review
Abstract
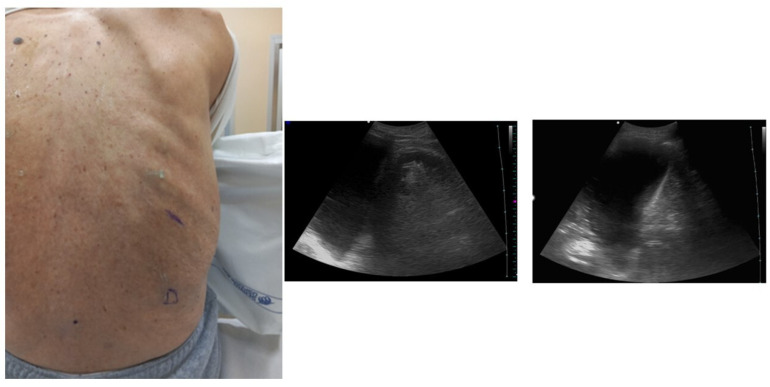
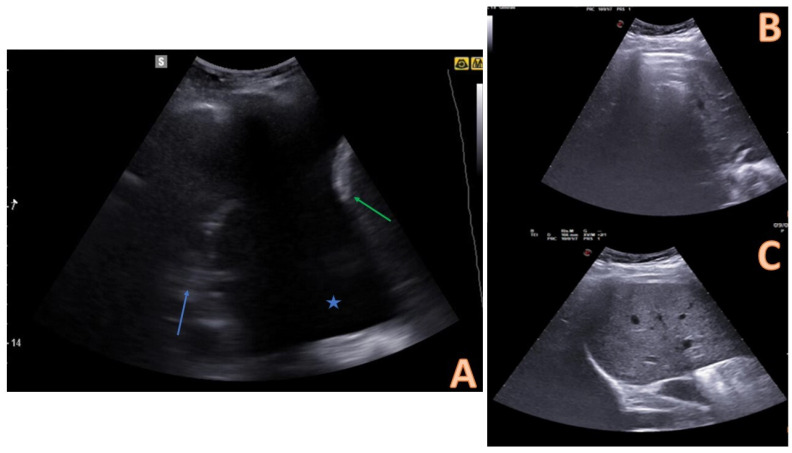
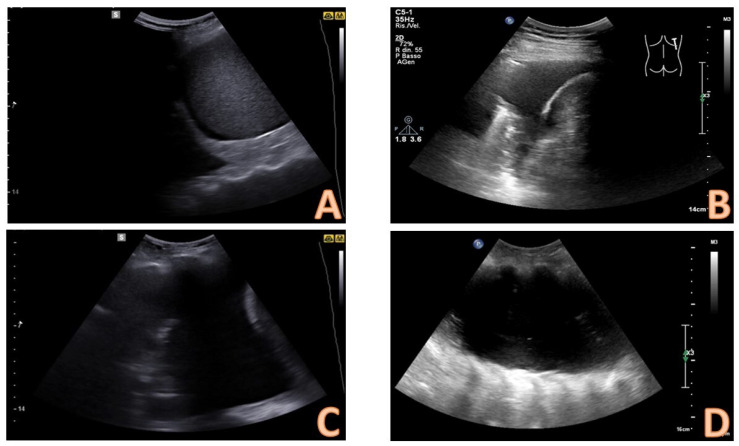
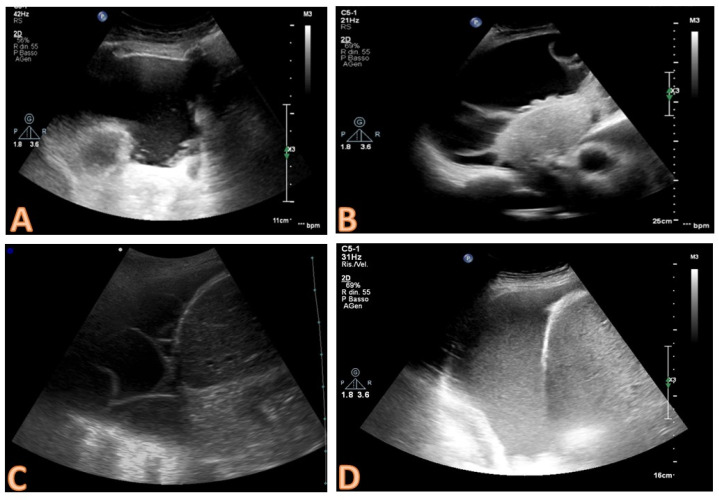
Thoracentesis is one of the most important invasive procedures in the clinical setting. Particularly, thoracentesis can be relevant in the evaluation of a new diagnosed pleural effusion, thus allowing for the collection of pleural fluid so that laboratory tests essential to establish a diagnosis can be performed. Furthermore, thoracentesis is a maneuver that can have therapeutic and palliative purposes. Historically, the procedure was performed based on a physical examination. In recent years, the role of ultrasound has been established as a valuable tool for assistance and guidance in the thoracentesis procedure. The use of ultrasound increases success rates and significantly reduces complications. The aim of this educational review is to provide a detailed and sequential examination of the procedure, focusing on the two main modalities, the ultrasound-assisted and ultrasound-guided form.
Keywords: invasive; lung; pleural effusion; procedure; thoracentesis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Cocco G., Boccatonda A., Rossi I., D‘Ardes D., Corvino A., Delli Pizzi A., Ucciferri C., Katia F., Jacopo V. Early detection of pleuro-pulmonary tuberculosis by bedside lung ultrasound: A case report and review of literature. Clin. Case Rep. 2022;10:e05739. doi: 10.1002/ccr3.5739. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
