

Effects of Targeted Hypercapnia on Mortality and Length of Stay of Post-cardiac Arrest Patients: A Systematic Review and Meta-Analysis
- PMID: 38894798
- PMCID: PMC11185866
- DOI: 10.7759/cureus.60617
Effects of Targeted Hypercapnia on Mortality and Length of Stay of Post-cardiac Arrest Patients: A Systematic Review and Meta-Analysis
Abstract
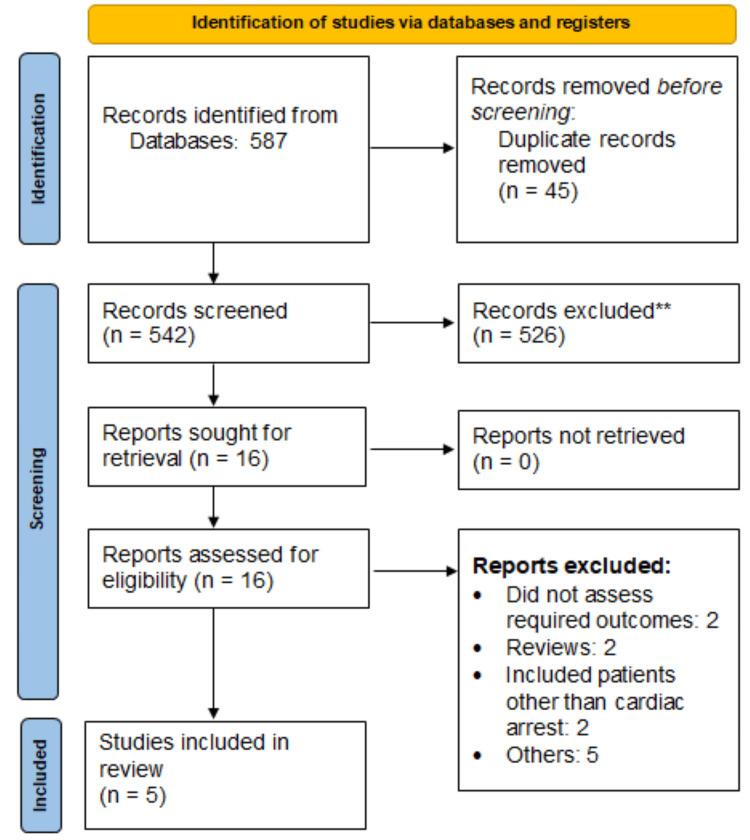
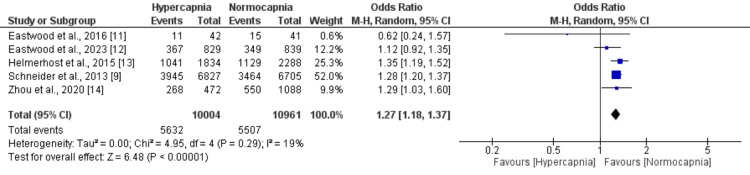
Therapeutic hypercapnia has been proposed as a potential strategy to enhance cerebral perfusion and improve outcomes in patients after cardiac arrest. However, the effects of targeted hypercapnia remain unclear. We conducted a systematic review and meta-analysis to evaluate the impact of hypercapnia compared to normocapnia on mortality and length of stay in post-cardiac arrest patients. We searched major databases for randomized controlled trials and observational studies comparing outcomes between hypercapnia and normocapnia in adult post-cardiac arrest patients. Data on in-hospital mortality and the ICU and hospital length of stay were extracted and pooled using random-effects meta-analysis. Five studies (two randomized controlled trials (RCTs) and three observational studies) with a total of 1,837 patients were included. Pooled analysis showed hypercapnia was associated with significantly higher in-hospital mortality compared to normocapnia (56.2% vs. 50.5%, OR 1.24, 95% CI 1.12-1.37, p<0.001). There was no significant heterogeneity (I2 = 25%, p = 0.26). No statistically significant differences were found for ICU length of stay (mean difference 0.72 days, 95% CI -0.51 to 1.95) or hospital length of stay (mean difference 1.13 days, 95% CI -0.67 to 2.93) between the groups. Sensitivity analysis restricted to mild hypercapnia studies did not alter the mortality findings. This meta-analysis did not find a mortality benefit with targeted hypercapnia compared to normocapnia in post-cardiac arrest patients. The results align with current guidelines recommending a normal partial pressure of arterial carbon dioxide (PaCO2) target range and do not support routinely targeting higher carbon dioxide levels in this setting.
Keywords: hypercapnia; length of stay; mortality; normocapnia; systematic review and meta-analysis.
Copyright © 2024, Damarlapally et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Impact of normocapnia vs. mild hypercapnia on prognosis after cardiac arrest: A systematic review and meta-analysis.Am J Emerg Med. 2025 Apr;90:1-8. doi: 10.1016/j.ajem.2024.12.060. Epub 2024 Dec 27. Am J Emerg Med. 2025. PMID: 39778435
-
Association between mild hypercapnia and hospital mortality in patients admitted to the intensive care unit after cardiac arrest: A retrospective study.Resuscitation. 2020 Apr;149:30-38. doi: 10.1016/j.resuscitation.2020.01.036. Epub 2020 Feb 11. Resuscitation. 2020. PMID: 32057947
-
Mild Hypercapnia or Normocapnia after Out-of-Hospital Cardiac Arrest.N Engl J Med. 2023 Jul 6;389(1):45-57. doi: 10.1056/NEJMoa2214552. Epub 2023 Jun 15. N Engl J Med. 2023. PMID: 37318140 Clinical Trial.
-
Association of Hypercapnia and Hypercapnic Acidosis With Clinical Outcomes in Mechanically Ventilated Patients With Cerebral Injury.JAMA Neurol. 2018 Jul 1;75(7):818-826. doi: 10.1001/jamaneurol.2018.0123. JAMA Neurol. 2018. PMID: 29554187 Free PMC article.
-
Association between arterial carbon dioxide tension and poor outcomes after cardiac arrest: A meta-analysis.Anaesth Crit Care Pain Med. 2025 May;44(3):101522. doi: 10.1016/j.accpm.2025.101522. Epub 2025 Apr 24. Anaesth Crit Care Pain Med. 2025. PMID: 40286876
References
-
- Neurologic function and health-related quality of life in patients following targeted temperature management at 33°C vs 36°C after out-of-hospital cardiac arrest: a randomized clinical trial. Cronberg T, Lilja G, Horn J, et al. JAMA Neurol. 2015;72:634–641. - PubMed
-
- Critical care of the post-cardiac arrest patient. Walker AC, Johnson NJ. Cardiol Clin. 2018;36:419–428. - PubMed
-
- Post cardiac arrest syndrome: a review of therapeutic strategies. Stub D, Bernard S, Duffy SJ, Kaye DM. Circulation. 2011;123:1428–1435. - PubMed
Publication types
LinkOut - more resources
Full Text Sources