

Efficacy of steroid therapy in the acute stage of anti-NMDAR and anti-MOG antibody overlapping encephalitis: a case report and literature review
- PMID: 38895128
- PMCID: PMC11184463
- DOI: 10.3389/fimmu.2024.1392992
Efficacy of steroid therapy in the acute stage of anti-NMDAR and anti-MOG antibody overlapping encephalitis: a case report and literature review
Abstract
Background: Recently, cases of overlapping encephalitis caused by anti-N-methyl-D-aspartate receptor (anti-NMDAR) and anti-myelin oligodendrocyte glycoprotein (MOG) antibodies have been reported, and their clinical characteristics are gradually becoming clear. Acute-phase treatment typically involves the use of steroids, and although some studies have suggested that steroids can be effective, the extent of their efficacy has not yet been fully explored.
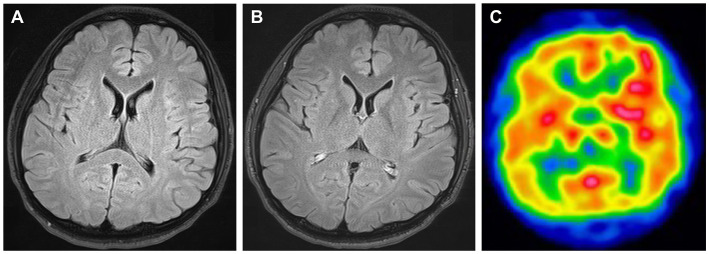
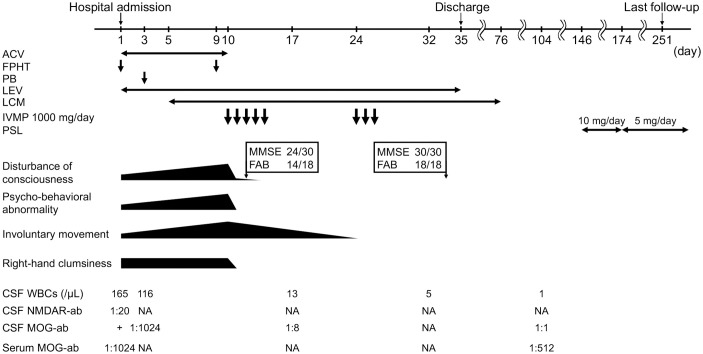
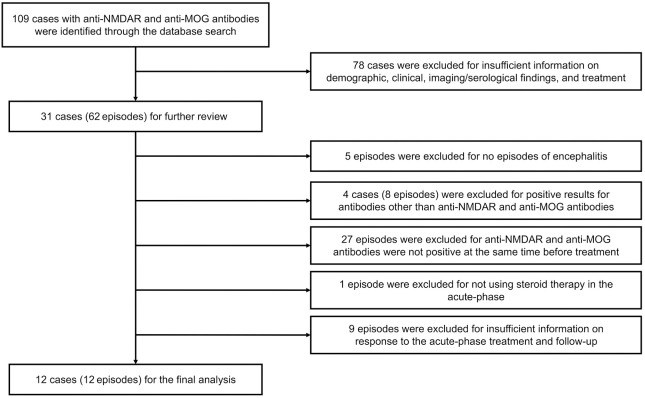
Case presentation: We present the case of a 25-year-old man with anti-NMDAR and anti-MOG antibody overlapping encephalitis who showed considerable improvement after steroid treatment. To gain a deeper understanding of the efficacy of steroids in managing this condition, we conducted a literature review of cases of anti-NMDAR and anti-MOG antibody double-positive encephalitis that were treated with steroids during the acute phase. Thirteen cases were analyzed, including a new case diagnosed at our hospital. All patients showed improvement after receiving steroid treatment in the acute phase. Ten patients did not have any sequelae, and nine of them showed a rapid or major response during the acute phase. In contrast, three patients experienced sequelae (mild cognitive decline, visual impairment, and memory impairment, respectively), with their response to steroids in the acute phase being slow or limited. Relapses occurred in five patients, in one patient during steroid tapering, and in another two patients after cessation of steroids.
Conclusion: Steroid therapy can be effective in the acute stage of anti-NMDAR and anti-MOG antibody overlapping encephalitis. A positive prognosis may be expected in patients who experience substantial improvement with steroid therapy during the acute phase.
Keywords: N-methyl-D-aspartate receptor (NMDAR); anti-NMDAR encephalitis; autoimmune encephalitis; myelin oligodendrocyte glycoprotein (MOG); overlapping encephalitis; steroid.
Copyright © 2024 Kondo, Takeuchi, Niwa, Yoshida, Takemura, Hosoyama, Kaga, Kaneko and Mabuchi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A rare concurrence: Antibodies against Myelin Oligodendrocyte Glycoprotein and N-methyl-d-aspartate receptor in a child.Mult Scler Relat Disord. 2019 Feb;28:101-103. doi: 10.1016/j.msard.2018.12.017. Epub 2018 Dec 14. Mult Scler Relat Disord. 2019. PMID: 30590238
-
Clinical characterization of diseases associated with anti-N-methyl-D-aspartate receptor encephalitis combined with anti-myelin oligodendrocyte glycoprotein antibodies in adults.J Neurol. 2025 Mar 12;272(4):262. doi: 10.1007/s00415-025-13011-5. J Neurol. 2025. PMID: 40072596
-
Clinical characteristics of children with anti-N-methyl-D-aspartate receptor encephalitis with and without anti-myelin oligodendrocyte glycoprotein antibody.Eur J Pediatr. 2025 Mar 14;184(4):249. doi: 10.1007/s00431-025-06078-9. Eur J Pediatr. 2025. PMID: 40082268
-
FLAMES overlaying anti-N-methyl-D-aspartate receptor encephalitis: a case report and literature review.BMC Neurol. 2024 Apr 25;24(1):140. doi: 10.1186/s12883-024-03617-z. BMC Neurol. 2024. PMID: 38664672 Free PMC article. Review.
-
Clinical features and management of coexisting anti-N-methyl-D-aspartate receptor encephalitis and myelin oligodendrocyte glycoprotein antibody-associated encephalomyelitis: a case report and review of the literature.Neurol Sci. 2021 Mar;42(3):847-855. doi: 10.1007/s10072-020-04942-0. Epub 2021 Jan 7. Neurol Sci. 2021. PMID: 33409829 Review.
Cited by
-
Successful sequential therapy with rituximab and telitacicept in refractory Anti-NMDA receptor encephalitis and MOG-associated demyelination: a case report and literature review.Front Immunol. 2025 Feb 6;16:1509143. doi: 10.3389/fimmu.2025.1509143. eCollection 2025. Front Immunol. 2025. PMID: 39981240 Free PMC article. Review.
-
Autoantibodies Against Collapsin Response Mediator Proteins Associated With Encephalopathy/Myelopathy: A Single-Center Retrospective Study.CNS Neurosci Ther. 2025 Jun;31(6):e70423. doi: 10.1111/cns.70423. CNS Neurosci Ther. 2025. PMID: 40583162 Free PMC article.
References
-
- Titulaer MJ, McCracken L, Gabilondo I, Armangué T, Glaser C, Iizuka T, et al. . Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. (2013) 12:157–65. doi: 10.1016/S1474-4422(12)70310-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources