

The impact of pre-rehydration guided by carotid corrected flow time on hypotension prevention following general anesthesia induction in patients undergoing gastrointestinal surgery: a prospective randomized controlled trial
- PMID: 38895180
- PMCID: PMC11184214
- DOI: 10.3389/fmed.2024.1416574
The impact of pre-rehydration guided by carotid corrected flow time on hypotension prevention following general anesthesia induction in patients undergoing gastrointestinal surgery: a prospective randomized controlled trial
Abstract
Background: Patients undergoing gastrointestinal surgery often experience hypotension following general anesthesia induction due to insufficient volume. This study aimed to assess whether pre-rehydration guided by carotid corrected flow time (FTc) could mitigate post-induction hypotension induced by general anesthesia.
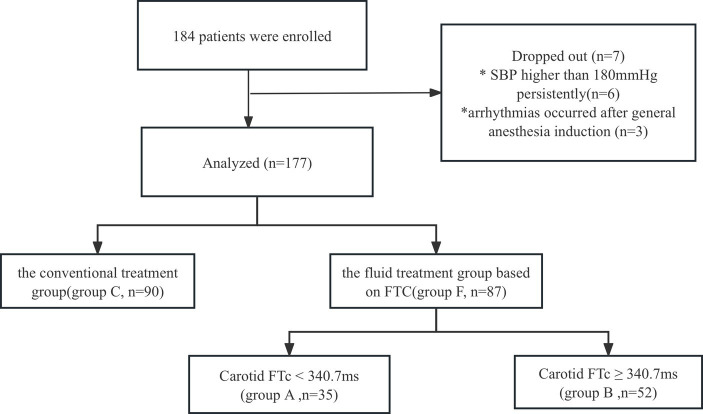
Methods: Patients undergoing resection of gastrointestinal tumors were assigned to either the conventional treatment group (Group C) or the fluid treatment group based on FTc (Group F). Within Group F, patients were further divided into Group A (carotid FTc <340.7 ms) and Group B (carotid FTc ≥340.7 ms) based on pre-rehydration carotid FTc values. Group A patients received pre-rehydration with 250 mL of colloids (hydroxyethyl starch-HES) administered within 15 min until carotid FTc reached ≥340.7 ms to counteract hypovolemia prior to induction. Patients in Group B and Group C received a continuous HES infusion at a rate of 6 mL/kg/h 30 min before induction to compensate for physiological fluid loss. All patients received a perioperative background infusion of 3 mL/kg/h compound sodium chloride, with infusion rates optimized based on mean arterial pressure (MAP) and heart rate (HR). The incidence of post-induction hypotension was compared between Group C and Group F, as well as between Group A and Group B.
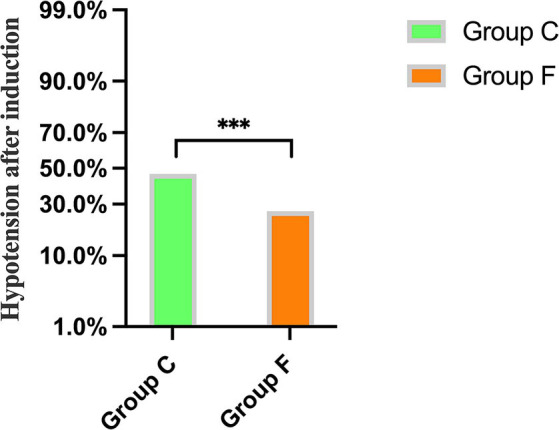
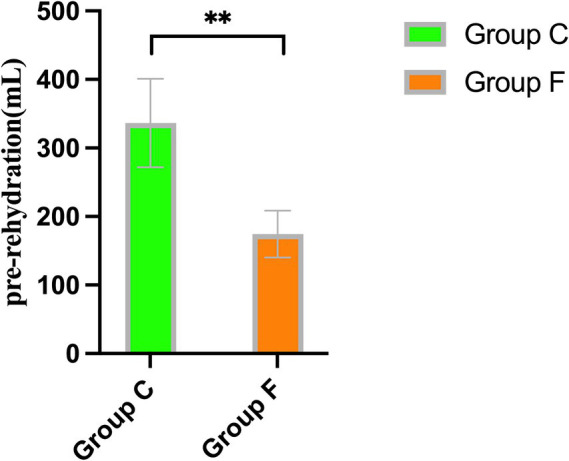
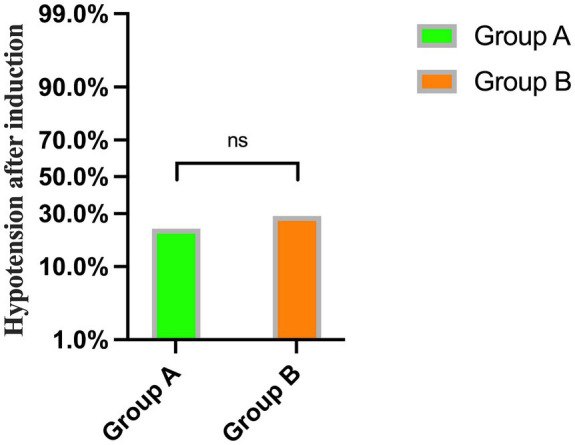
Results: The incidence of hypotension after induction was significantly lower in Group F compared to Group C (26.4% vs. 46.7%, respectively; p < 0.001). Patients in Group A received significantly more pre-rehydration, leading to a greater increase in carotid FTc values compared to Group B (336.5 ± 64.5 vs. 174.3 ± 34.1 ms, p = 0.002). However, no significant difference in carotid FTc values after pre-rehydration was observed between the groups. There was no significant difference in the incidence of hypotension after general anesthesia induction between Group A and Group B (22.9% vs. 28.8%, p = 0.535).
Conclusion: Pre-rehydration based on FTc can effectively reduce the occurrence of post-induction hypotension in patients undergoing gastrointestinal surgery who present with insufficient volume.
Clinical trial registration: https://www.chictr.org.cn/showprojEN.html?proj=201481.
Keywords: carotid corrected flow time; gastrointestinal surgery; general anesthesia; hypotension; pre-rehydration.
Copyright © 2024 Li, Li, Yu, Tang, Zhou, Chen and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effect of carotid corrected flow time combined with perioperative fluid therapy on preventing hypotension after general anesthesia induction in elderly patients: a prospective cohort study.Int J Surg. 2024 Feb 1;110(2):799-809. doi: 10.1097/JS9.0000000000000863. Int J Surg. 2024. PMID: 37983823 Free PMC article.
-
Carotid artery corrected flow time and respiratory variations of peak blood flow velocity for prediction of hypotension after induction of general anesthesia in elderly patients.BMC Geriatr. 2022 Nov 19;22(1):882. doi: 10.1186/s12877-022-03619-x. BMC Geriatr. 2022. PMID: 36402973 Free PMC article.
-
The effects of crystalloid and colloid preload on cardiac output in the parturient undergoing planned cesarean delivery under spinal anesthesia: a randomized trial.Anesth Analg. 2009 Dec;109(6):1916-21. doi: 10.1213/ANE.0b013e3181bbfdf6. Anesth Analg. 2009. PMID: 19923521 Clinical Trial.
-
Norepinephrine in Goal-Directed Fluid Therapy During General Anesthesia in Elderly Patients Undergoing Spinal Operation: Determining Effective Infusion Rate to Enhance Postoperative Functions.Curr Genomics. 2021 Dec 31;22(8):620-629. doi: 10.2174/1389202922666211213104944. Curr Genomics. 2021. PMID: 35386191 Free PMC article. Review.
-
Diagnostic Efficacy of Carotid Ultrasound for Predicting the Risk of Perioperative Hypotension or Fluid Responsiveness: A Meta-Analysis.Diagnostics (Basel). 2023 Jul 6;13(13):2290. doi: 10.3390/diagnostics13132290. Diagnostics (Basel). 2023. PMID: 37443683 Free PMC article. Review.
References
-
- Huang S, Liao Z, Chen A, Wang J, Xu X, Zhang L. Effect of carotid corrected flow time combined with perioperative fluid therapy on preventing hypotension after general anesthesia induction in elderly patients: a prospective cohort study. Int J Surg. (2024) 110:799–809. doi: 10.1097/JS9.0000000000000863 - DOI - PMC - PubMed
-
- Lee Y-H, Jang H-W, Park C-H, An S-M, Lee E-K, Choi B-M, et al. . Changes in plasma volume before and after major abdominal surgery following stroke volume variation-guided fluid therapy: a randomized controlled trial. Minerva Anestesiol. (2020) 86:507–17. doi: 10.23736/S0375-9393.19.13952-1, PMID: - DOI - PubMed
-
- Jun JH, Chung RK, Baik HJ, Chung MH, Hyeon JS, Lee YG, et al. . The tidal volume challenge improves the reliability of dynamic preload indices during robot-assisted laparoscopic surgery in the Trendelenburg position with lung-protective ventilation. BMC Anesthesiol. (2019) 19:142. doi: 10.1186/s12871-019-0807-6, PMID: - DOI - PMC - PubMed
-
- Alvarado Sánchez JI, Caicedo Ruiz JD, Diaztagle Fernández JJ, Ospina-Tascón GA, Cruz Martínez LE. Use of pulse pressure variation as predictor of fluid responsiveness in patients ventilated with low tidal volume: a systematic review and Meta-analysis. Clin Med Insights Circ Respir Pulm Med. (2020) 14:1179548420901518. doi: 10.1177/1179548420901518, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources