

Optimizing accrual to a large-scale, clinically integrated randomized trial in anesthesiology: A 2-year analysis of recruitment
- PMID: 38895970
- PMCID: PMC11655704
- DOI: 10.1177/17407745241255087
Optimizing accrual to a large-scale, clinically integrated randomized trial in anesthesiology: A 2-year analysis of recruitment
Abstract
Background: Performing large randomized trials in anesthesiology is often challenging and costly. The clinically integrated randomized trial is characterized by simplified logistics embedded into routine clinical practice, enabling ease and efficiency of recruitment, offering an opportunity for clinicians to conduct large, high-quality randomized trials under low cost. Our aims were to (1) demonstrate the feasibility of the clinically integrated trial design in a high-volume anesthesiology practice and (2) assess whether trial quality improvement interventions led to more balanced accrual among study arms and improved trial compliance over time.
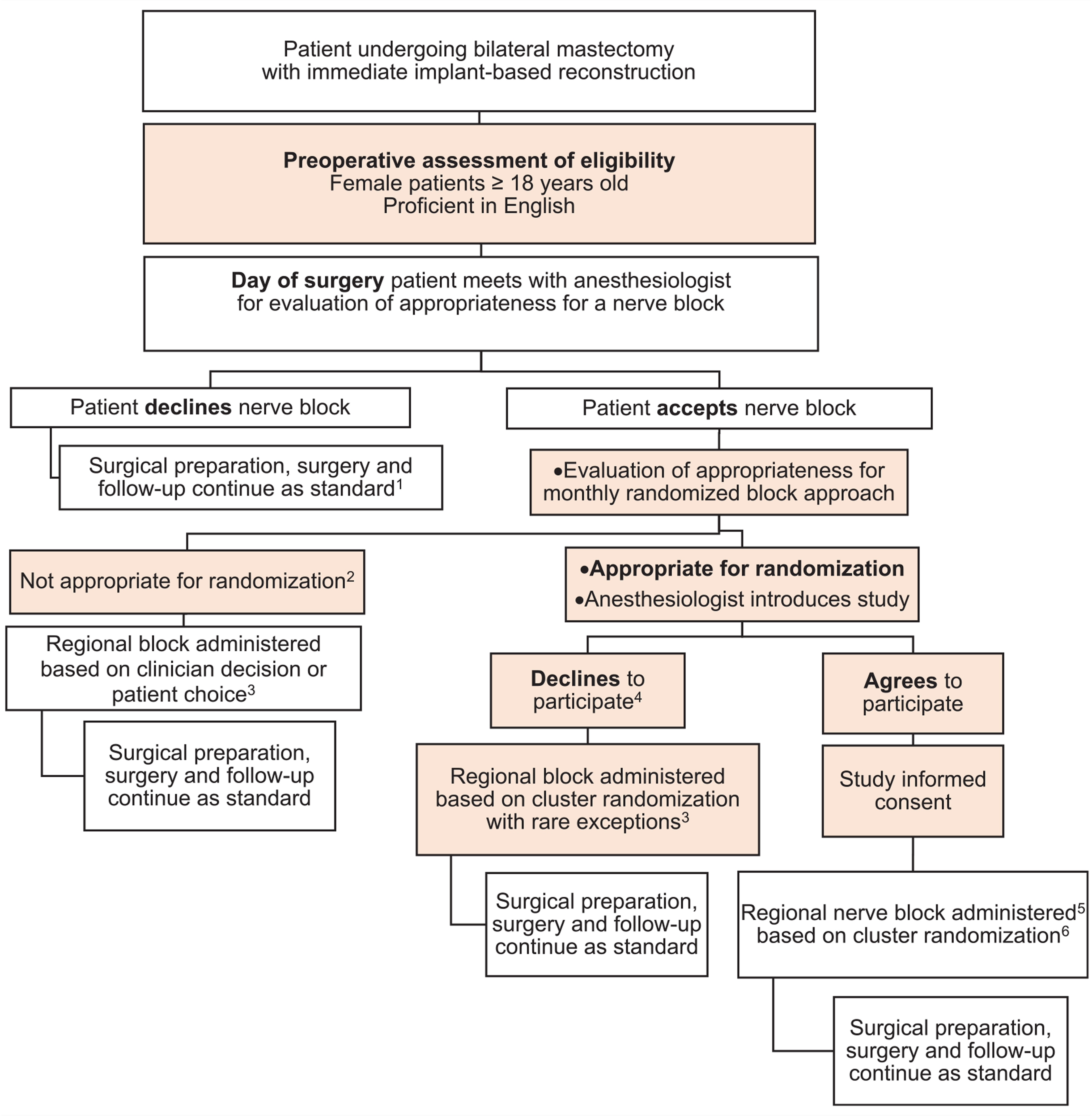
Methods: This is an interim analysis of recruitment to a cluster-randomized trial investigating three nerve block approaches for mastectomy with immediate implant-based reconstruction: paravertebral block (arm 1), paravertebral plus interpectoral plane blocks (arm 2), and serratus anterior plane plus interpectoral plane blocks (arm 3). We monitored accrual and consent rates, clinician compliance with the randomized treatment, and availability of outcome data. Assessment after the initial year of implementation showed a slight imbalance in study arms suggesting areas for improvement in trial compliance. Specific improvement interventions included increasing the frequency of communication with the consenting staff and providing direct feedback to clinician investigators about their individual recruitment patterns. We assessed overall accrual rates and tested for differences in accrual, consent, and compliance rates pre- and post-improvement interventions.
Results: Overall recruitment was extremely high, accruing close to 90% of the eligible population. In the pre-intervention period, there was evidence of bias in the proportion of patients being accrued and receiving the monthly block, with higher rates in arm 3 (90%) compared to arms 1 (81%) and 2 (79%, p = 0.021). In contrast, in the post-intervention period, there was no statistically significant difference between groups (p = 0.8). Eligible for randomization rate increased from 89% in the pre-intervention period to 95% in the post-intervention period (difference 5.7%; 95% confidence interval = 2.2%-9.4%, p = 0.002). Consent rate increased from 95% to 98% (difference of 3.7%; 95% confidence interval = 1.1%-6.3%; p = 0.004). Compliance with the randomized nerve block approach was maintained at close to 100% and availability of primary outcome data was 100%.
Conclusion: The clinically integrated randomized trial design enables rapid trial accrual with a high participant compliance rate in a high-volume anesthesiology practice. Continuous monitoring of accrual, consent, and compliance rates is necessary to maintain and improve trial conduct and reduce potential biases. This trial methodology serves as a template for the implementation of other large, low-cost randomized trials in anesthesiology.
Keywords: Clinically-integrated randomized trial; day of surgery consent; high accrual; low cost trial; point of care randomization; pragmatic trial; recruitment analysis; regional anesthesia.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Safety and Efficacy of Imatinib for Hospitalized Adults with COVID-19: A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Oct 28;21(1):897. doi: 10.1186/s13063-020-04819-9. Trials. 2020. PMID: 33115543 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Accrual Quality Improvement Program for clinical trials.Clin Trials. 2024 Dec;21(6):744-753. doi: 10.1177/17407745241243027. Epub 2024 Apr 9. Clin Trials. 2024. PMID: 38591816 Free PMC article.
-
Electronic self-reporting of adverse events for patients undergoing cancer treatment: the eRAPID research programme including two RCTs.Southampton (UK): NIHR Journals Library; 2022 Feb. Southampton (UK): NIHR Journals Library; 2022 Feb. PMID: 35138783 Free Books & Documents. Review.
-
Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. PMID: 30354042 Free Books & Documents. Review.
Cited by
-
Successful completion of large, low-cost randomized cancer trials at an academic cancer center.Clin Trials. 2025 Feb;22(1):36-44. doi: 10.1177/17407745241284044. Epub 2024 Oct 15. Clin Trials. 2025. PMID: 39410769 Free PMC article.
References
-
- Goerke K, Parke M, Horn J, et al. Are results from randomized trials in anesthesiology robust or fragile? An analysis using the fragility index. Int J Evid Based Healthc 2020; 18(1): 116–124. - PubMed
-
- Turbitt LR, Mariano ER and El-Boghdadly K. Future directions in regional anaesthesia: not just for the cognoscenti. Anaesthesia 2020; 75: 293–297. - PubMed
-
- Albrecht E and Chin KJ. Advances in regional anaesthesia and acute pain management: a narrative review. Anaesthesia 2020; 75(Suppl. 1): e101–e110. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
