

18q Deletion Syndrome Presenting with Late-Onset Combined Immunodeficiency
- PMID: 38896123
- PMCID: PMC11186878
- DOI: 10.1007/s10875-024-01751-4
18q Deletion Syndrome Presenting with Late-Onset Combined Immunodeficiency
Abstract
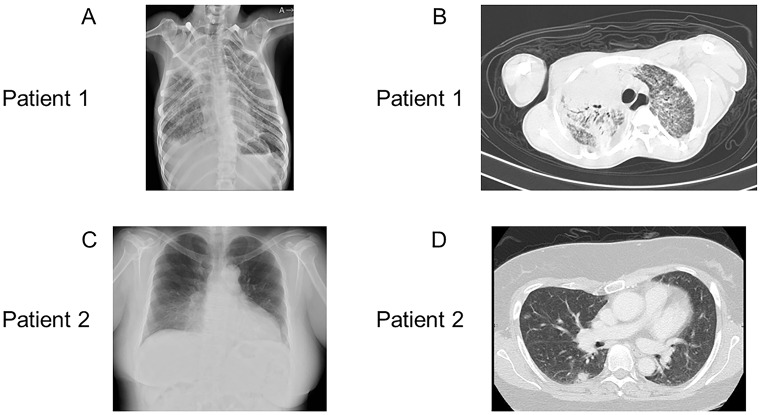
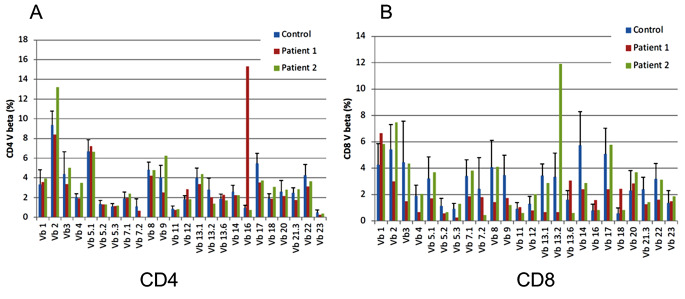
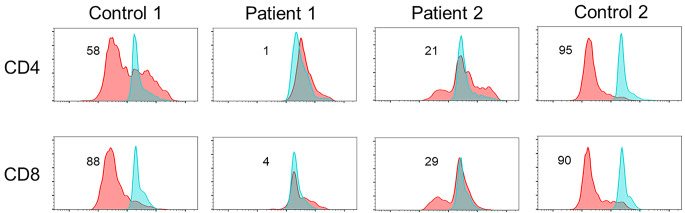
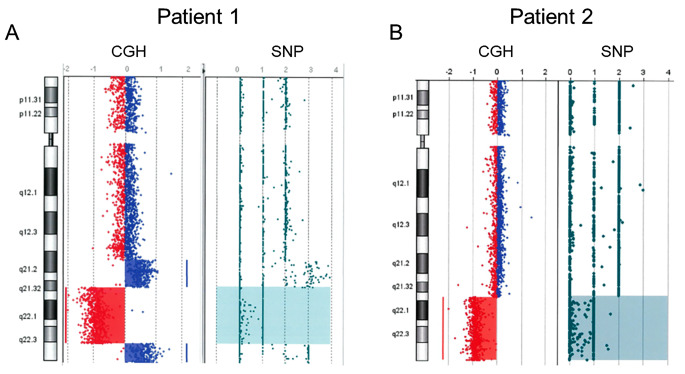
Patients with chromosome 18q deletion syndrome generally experience hypogammaglobulinemia. Herein, we describe two patients with chromosome 18q deletion syndrome who presented with late-onset combined immune deficiency (LOCID), which has not been previously reported. Patient 1 was a 29-year-old male with 18q deletion syndrome, who was being managed for severe motor and intellectual disabilities at the Yamabiko Medical Welfare Center for 26 years. Although the patient had few infections, he developed Pneumocystis pneumonia at the age of 28. Patient 2, a 48-year-old female with intellectual disability and congenital malformations, was referred to Tokyo Medical and Dental University Hospital with abnormal bilateral lung shadows detected on her chest radiography. Computed tomography showed multiple lymphadenopathies and pneumonia. A lymph node biopsy of the inguinal region revealed granulomatous lymphadenitis, and a chromosomal examination revealed 18q deletion. Array-based genomic hybridization analysis revealed deletion at 18q21.32-q22.3 for patient 1 and at 18q21.33-qter for patient 2. Immune status work-up of the two patients revealed panhypogammaglobulinemia, decreased number of memory B cells and naïve CD4+ and/or CD8+ cells, reduced response on the carboxyfluorescein diacetate succinimidyl ester T-cell division test, and low levels of T-cell receptor recombination excision circles and Ig κ-deleting recombination excision circles. Consequently, both patients were diagnosed with LOCID. Although patients with 18q deletion syndrome generally experience humoral immunodeficiency, the disease can be further complicated by cell-mediated immunodeficiency, causing combined immunodeficiency. Therefore, patients with 18q deletion syndrome should be regularly tested for cellular/humoral immunocompetence.
Keywords: Pneumocystis pneumonia; 18q deletion syndrome; Array-based comparative genomic hybridization; Common variable immunodeficiency; Late-onset combined immunodeficiency.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- De Grouchy J, Royer P, Salmon C, Lamy M. Partial deletion of the long arms of the chromosome 18. Pathol Biol. 1964;12:579–82. - PubMed
-
- Hogendorf A, Zieliński M, Constantinou M, Smigiel R, Wierzba J, Wyka K, et al. Immune dysregulation in patients with chromosome 18q deletions-searching for putative loci for autoimmunity and immunodeficiency. Front Immunol. 2021;12:742834. 10.3389/fimmu.2021.742834. 10.3389/fimmu.2021.742834 - DOI - PMC - PubMed
-
- Slyper AH, Pietryga D. Conversion of selective IgA deficiency to common variable immunodeficiency in an adolescent female with 18q deletion syndrome. Eur J Pediatr. 1997;156:155–6. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials
