

Multi-level tuberculosis of the spine identified by 18 F-FDG-PET/CT and concomitant urogenital tuberculosis: a case report from the spinal TB X cohort
- PMID: 38896371
- PMCID: PMC11621135
- DOI: 10.1007/s15010-024-02327-5
Multi-level tuberculosis of the spine identified by 18 F-FDG-PET/CT and concomitant urogenital tuberculosis: a case report from the spinal TB X cohort
Abstract
Background: Tuberculosis (TB) is caused by Mycobacterium tuberculosis (Mtb) and typically infects the lungs. However, extrapulmonary forms of TB can be found in approximately 20% of cases. It is suggested, that up to 10% of extrapulmonary TB affects the musculoskeletal system, in which spinal elements (spinal tuberculosis, STB) are involved in approximately 50% of the cases. STB is a debilitating disease with nonspecific symptoms and diagnosis is often delayed for months to years. In our Spinal TB X Cohort, we aim to describe the clinical phenotype of STB using whole-body 18 F-fluorodeoxyglucose positron emission tomography computed tomography (PET/CT) and to identify a specific gene expression profile for the different stages of dissemination on PET/CT. Here we report on the first patient recruited into our cohort who underwent PET/CT before treatment initiation, at 6-months and at 12-months - time of TB treatment completion.
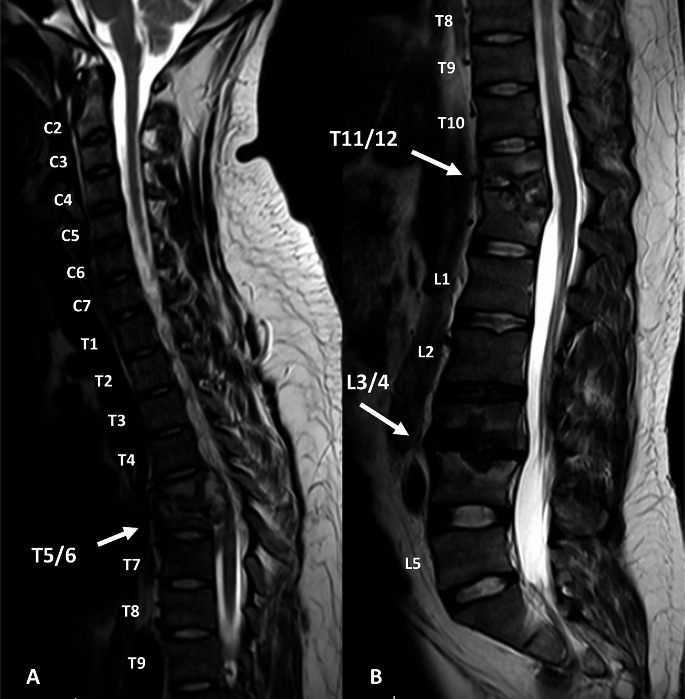
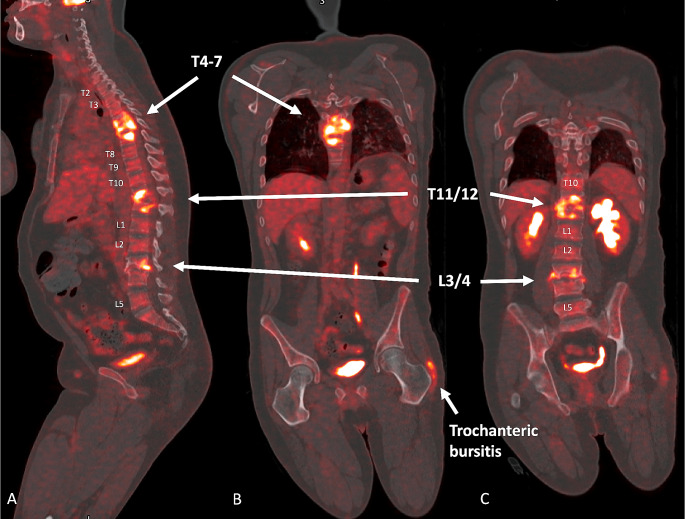
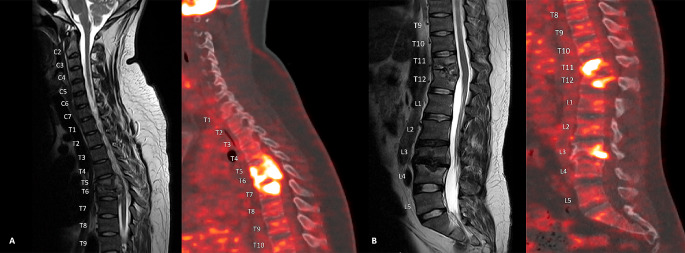
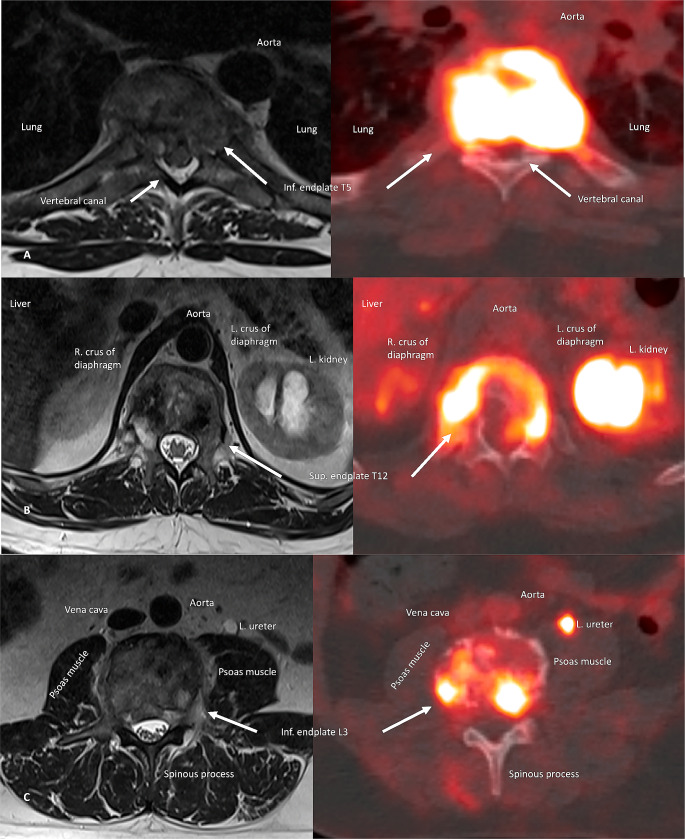
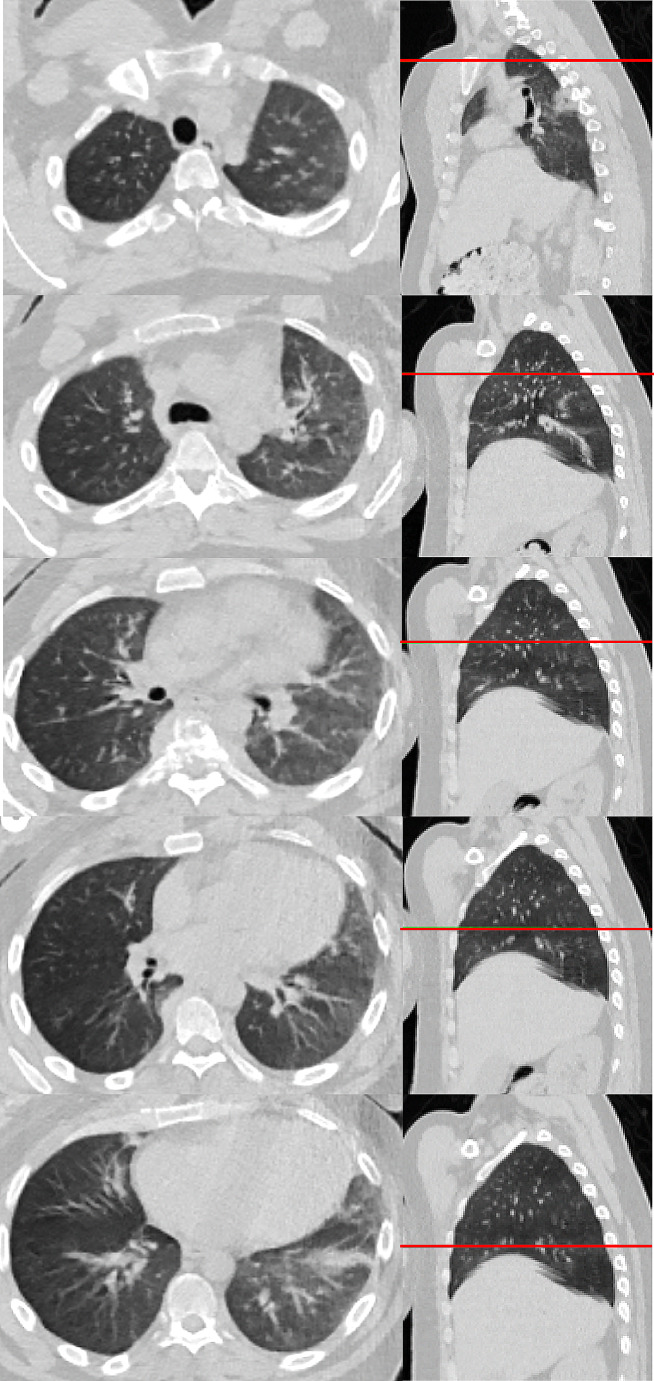
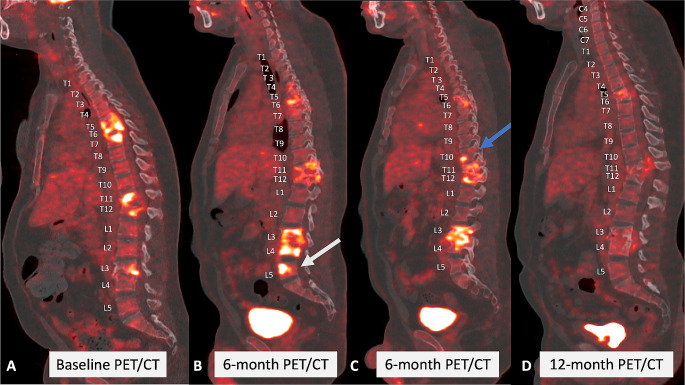
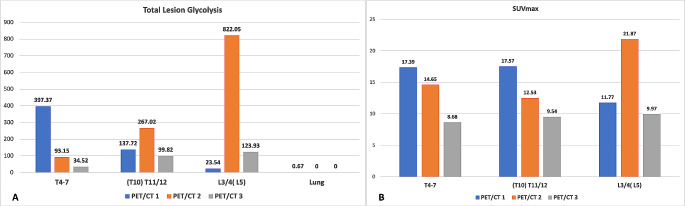
Case presentation: A 27-year-old immunocompetent male presented with severe thoracolumbar back pain for 9 months with severe antalgic gait and night sweats. Magnetic resonance imaging (MRI) of the whole spine revealed multilevel spinal disease (T5/6, T11/12, L3/4) in keeping with STB. After informed consent and recruitment into the Spinal TB X Cohort, the patient underwent PET/CT as per protocol, which revealed isolated multilevel STB (T4-7, T11/12, L3/4) with no concomitant lung or urogenital lesion. However, sputum and urine were Xpert MTB/RIF Ultra positive and Mtb was cultured from the urine sample. CT-guided biopsy of the T11/12 lesion confirmed drug-sensitive Mtb on Xpert MTB/RIF Ultra and the patient was started on TB treatment according to local guidelines for 12 months. The 6-month follow-up PET/CT revealed new and existing spinal lesions with increased FDG-uptake despite significant improvement of clinical features and laboratory markers. After 9 months of treatment, the patient developed an acute urethral stricture, most likely due to urogenital TB, and a suprapubic catheter was inserted. The 12-month PET/CT showed significantly decreased PET/CT values of all lesions, however, significant persistent spinal inflammation was present at the end of TB treatment. Clinically, the patient was considered cured by the TB control program and currently awaits urethroplasty.
Conclusions: In our case, PET/CT emerged as a valuable imaging modality for the initial assessment, surpassing MRI by revealing more comprehensive extensive disease. Subsequent PET/CT scans at 6-month uncovered new lesions and increased inflammation in existing ones, while by the end of TB treatment, all lesions exhibited improvement. However, the interpretation of FDG avidity remains ambiguous, whether it correlates with active infection and viable Mtb. or fibro- and osteoblast activity indicative of the healing process. Additionally, the absence of extraspinal TB lesions on PET/CT despite positive microbiology from sputum and urine maybe explained by paucibacillary, subclinical infection of extraspinal organs. The Spinal TB X Cohort endeavours to shed light on whole-body imaging patterns at diagnosis, their evolution midway through TB treatment, and upon treatment completion. Ultimately, this study aims to advance our understanding of the biology of this complex disease.
Keywords: 18F-FDG-PET/CT; Infection; PET/CT; Pott’s disease; Spine; Spondylodiscitis; TB; Tuberculous spondylodiscitis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: The University of Cape Town Ethics Committee approved the Spinal TB X cohort (HREC:243/2022). The study has been registered on ClinicalTrials.gov (NCT05610098). Consent to participate: All participants from the Spinal TB X cohort undergo written informed consent before inclusion. Consent to publish: The participant in this study has signed the written consent for publication. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Comparing gene expression profiles of adults with isolated spinal tuberculosis to disseminated spinal tuberculosis identified by 18FDG-PET/CT at time of diagnosis, 6- and 12-months follow-up: classifying clinical stages of spinal tuberculosis and monitoring treatment response (Spinal TB X cohort study).J Orthop Surg Res. 2024 Jun 25;19(1):376. doi: 10.1186/s13018-024-04840-7. J Orthop Surg Res. 2024. PMID: 38918806 Free PMC article.
-
PET-CT-guided characterisation of progressive, preclinical tuberculosis infection and its association with low-level circulating Mycobacterium tuberculosis DNA in household contacts in Leicester, UK: a prospective cohort study.Lancet Microbe. 2024 Feb;5(2):e119-e130. doi: 10.1016/S2666-5247(23)00289-6. Epub 2024 Jan 17. Lancet Microbe. 2024. PMID: 38244554
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Towards more accurate 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) imaging in active and latent tuberculosis.Int J Infect Dis. 2020 Mar;92S:S85-S90. doi: 10.1016/j.ijid.2020.02.017. Epub 2020 Feb 27. Int J Infect Dis. 2020. PMID: 32114199 Review.
-
Tuberculosis.Semin Nucl Med. 2018 Mar;48(2):108-130. doi: 10.1053/j.semnuclmed.2017.10.005. Epub 2017 Nov 16. Semin Nucl Med. 2018. PMID: 29452616 Review.
References
-
- World Health O. Global tuberculosis report 2022. Geneva: World Health Organization; 2022.
-
- Zumla A, Raviglione M, Hafner R. Fordham Von Reyn C. Tuberculosis. N Engl J Med. 2013;368:745–55. - PubMed
-
- European Centre for Disease Prevention and Control, WHO Regional Office for Europe. Tuberculosis surveillance and monitoring in Europe 2022–2020 data. Copenhagen: WHO Regional Office for Europe and Stockholm: European Centre for Disease Prevention and Control;; 2022. Licence: CC BY 3.0 IGO.
-
- Dunn RN, Husien MB. Spinal tuberculosis. Bone Joint J. 2018;100–B:425–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
