

Unmasking the hidden aftermath: postintensive care unit sequelae, discharge preparedness, and long-term follow-up
- PMID: 38896724
- PMCID: PMC11152445
- DOI: 10.62675/2965-2774.20240265-en
Unmasking the hidden aftermath: postintensive care unit sequelae, discharge preparedness, and long-term follow-up
Abstract
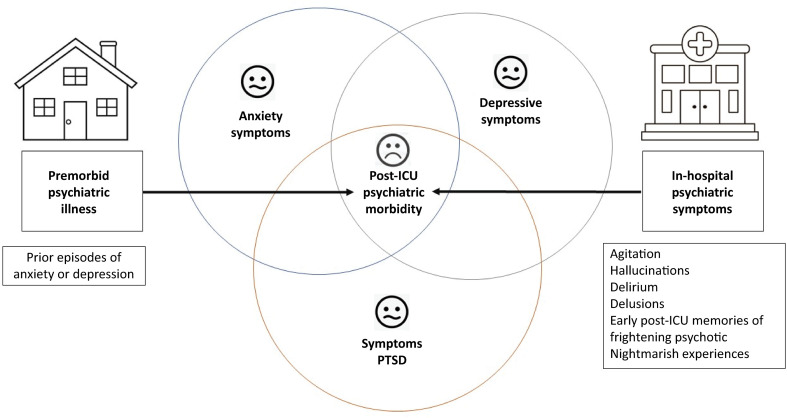
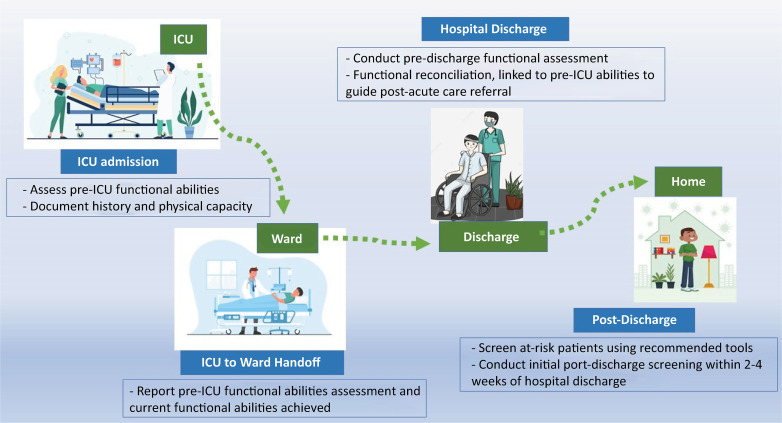
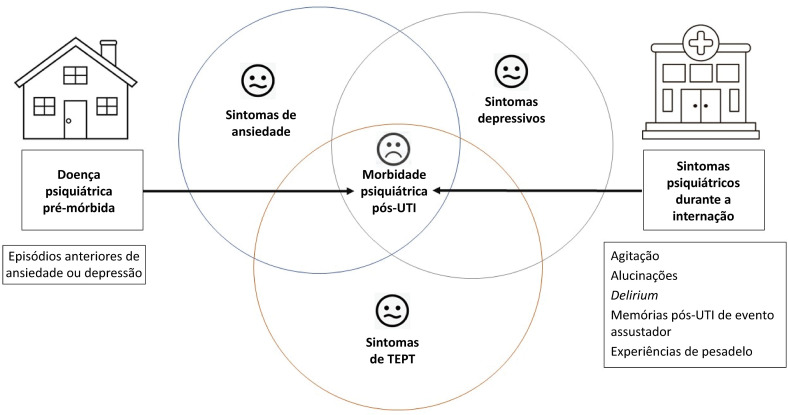
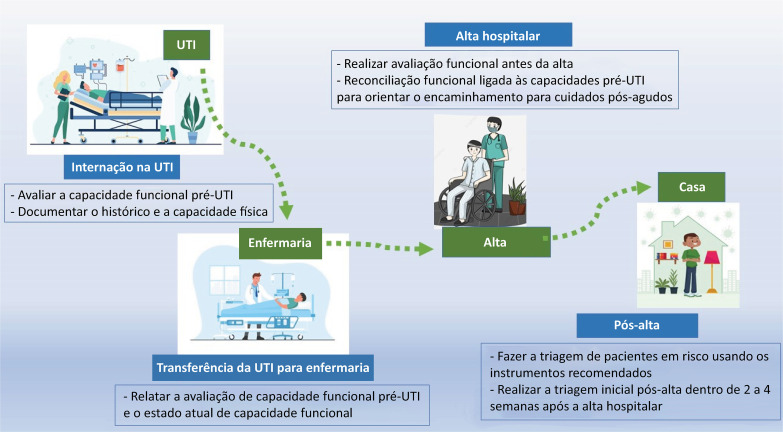
A significant portion of individuals who have experienced critical illness encounter new or exacerbated impairments in their physical, cognitive, or mental health, commonly referred to as postintensive care syndrome. Moreover, those who survive critical illness often face an increased risk of adverse consequences, including infections, major cardiovascular events, readmissions, and elevated mortality rates, during the months following hospitalization. These findings emphasize the critical necessity for effective prevention and management of long-term health deterioration in the critical care environment. Although conclusive evidence from well-designed randomized clinical trials is somewhat limited, potential interventions include strategies such as limiting sedation, early mobilization, maintaining family presence during the intensive care unit stay, implementing multicomponent transition programs (from intensive care unit to ward and from hospital to home), and offering specialized posthospital discharge follow-up. This review seeks to provide a concise summary of recent medical literature concerning long-term outcomes following critical illness and highlight potential approaches for preventing and addressing health decline in critical care survivors.
RESUMO: Parcela significativa de indivíduos que enfrentaram doença crítica sofre de síndrome pós-cuidados intensivos, caracterizada por comprometimento novo ou exacerbado da função física, cognitiva ou de saúde mental. Além disso, os sobreviventes geralmente apresentam maior risco de consequências adversas, como infecção, eventos cardiovasculares maiores, reinternação e taxas de mortalidade elevadas, durante os meses após a hospitalização. Esses achados reforçam a necessidade urgente de prevenção e manejo eficazes da deterioração da saúde a longo prazo no ambiente de cuidados intensivos. Embora haja poucas evidências conclusivas de ensaios clínicos randomizados bem desenhados, potenciais intervenções incluem estratégias como limitação da sedação, mobilização precoce, presença da família durante a internação na unidade de terapia intensiva, implementação de programas de transição multidisciplinares (da unidade de terapia intensiva para a enfermaria e do hospital para o domicílio) e acompanhamento especializado após a alta hospitalar. Esta revisão objetiva fornecer um resumo conciso da literatura médica recente sobre os desfechos a longo prazo após doenças críticas e destacar potenciais abordagens para prevenir e abordar a deterioração da saúde de sobreviventes de cuidados intensivos.
Conflict of interest statement
Figures
References
-
- Zampieri FG, Salluh JI, Azevedo LC, Kahn JM, Damiani LP, Borges LP, Viana WN, Costa R, Corrêa TD, Araya DE, Maia MO, Ferez MA, Carvalho AG, Knibel MF, Melo UO, Santino MS, Lisboa T, Caser EB, Besen BA, Bozza FA, Angus DC, Soares M, ORCHESTRA Study Investigators ICU staffing feature phenotypes and their relationship with patients' outcomes: an unsupervised machine learning analysis. Intensive Care Med. 2019;45(11):1599–1607. - PubMed
-
- Ludmir J, Netzer G. Family-centered care in the intensive care unit-what does best practice tell us? Semin Respir Crit Care Med. 2019;40(5):648–654. - PubMed
-
- Zimmerman JJ, Harmon LA, Smithburger PL, Chaykosky D, Heffner AC, Hravnak M, et al. Choosing wisely for critical care: the next five. Crit Care Med. 2021;49(3):472–481. - PubMed
-
- Writing Group for the CHECKLIST-ICU Investigators and the Brazilian Research in Intensive Care Network (BRICNet) Cavalcanti AB, Bozza FA, Machado FR, Salluh JI, Campagnucci VP, Vendramim P, et al. Effect of a quality improvement intervention with daily round checklists, goal setting, and clinician prompting on mortality of critically ill patients: a randomized clinical trial. JAMA. 2016;315(14):1480–1490. - PubMed
-
- Donovan AL, Aldrich J, Gross AK, Barchas DM, Thornton KC, Schell-Chaple HM, Gropper MA, Lipshutz AKM, University of California, San Francisco Critical Care Innovations Group Interprofessional care and teamwork in the ICU. Crit Care Med. 2018;46(6):980–990. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
