

Spatial Transcriptome-Wide Profiling of Small Cell Lung Cancer Reveals Intra-Tumoral Molecular and Subtype Heterogeneity
- PMID: 38896789
- PMCID: PMC11336901
- DOI: 10.1002/advs.202402716
Spatial Transcriptome-Wide Profiling of Small Cell Lung Cancer Reveals Intra-Tumoral Molecular and Subtype Heterogeneity
Abstract
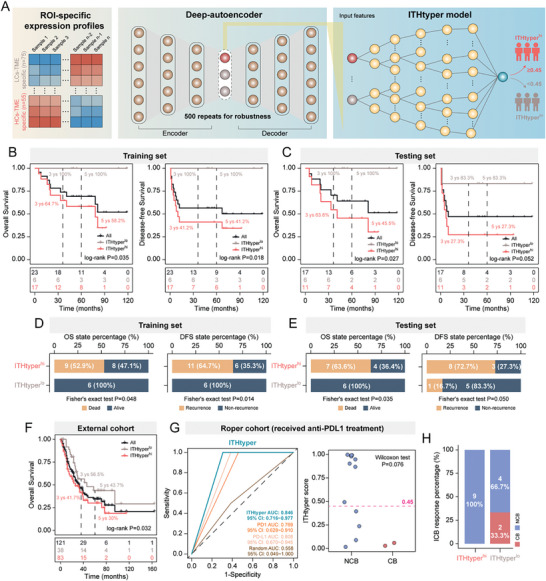
Small cell lung cancer (SCLC) is a highly aggressive malignancy characterized by rapid growth and early metastasis and is susceptible to treatment resistance and recurrence. Understanding the intra-tumoral spatial heterogeneity in SCLC is crucial for improving patient outcomes and clinically relevant subtyping. In this study, a spatial whole transcriptome-wide analysis of 25 SCLC patients at sub-histological resolution using GeoMx Digital Spatial Profiling technology is performed. This analysis deciphered intra-tumoral multi-regional heterogeneity, characterized by distinct molecular profiles, biological functions, immune features, and molecular subtypes within spatially localized histological regions. Connections between different transcript-defined intra-tumoral phenotypes and their impact on patient survival and therapeutic response are also established. Finally, a gene signature, termed ITHtyper, based on the prevalence of intra-tumoral heterogeneity levels, which enables patient risk stratification from bulk RNA-seq profiles is identified. The prognostic value of ITHtyper is rigorously validated in independent multicenter patient cohorts. This study introduces a preliminary tumor-centric, regionally targeted spatial transcriptome resource that sheds light on previously unexplored intra-tumoral spatial heterogeneity in SCLC. These findings hold promise to improve tumor reclassification and facilitate the development of personalized treatments for SCLC patients.
Keywords: digital spatial profiling (DSP); intra‐tumoral heterogeneity (ITH); small cell lung cancer (SCLC); spatial transcriptomics.
© 2024 The Author(s). Advanced Science published by Wiley‐VCH GmbH.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Horn L., Mansfield A. S., Szczęsna A., Havel L., Krzakowski M., Hochmair M. J., Huemer F., Losonczy G., Johnson M. L., Nishio M., Reck M., Mok T., Lam S., Shames D. S., Liu J., Ding B., Lopez‐Chavez A., Kabbinavar F., Lin W., Sandler A., Liu S. V., N. Engl. J. Med. 2018, 379, 2220. - PubMed
-
- Waqar S. N., Morgensztern D., Pharmacol. Ther. 2017, 180, 16. - PubMed
-
- a) Fisher R., Pusztai L., Swanton C., Br. J. Cancer 2013, 108, 479; - PMC - PubMed
- b) Marusyk A., Janiszewska M., Polyak K., Cancer Cell 2020, 37, 471; - PMC - PubMed
- c) McGranahan N., Swanton C., Cancer Cell 2015, 27, 15; - PubMed
- d) McGranahan N., Swanton C. J. C. c., Cancer Cell 2015, 27, 15. - PubMed
-
- George J., Lim J. S., Jang S. J., Cun Y., Ozretić L., Kong G., Leenders F., Lu X., Fernández‐Cuesta L., Bosco G., Müller C., Dahmen I., Jahchan N. S., Park K.‐S., Yang D., Karnezis A. N., Vaka D., Torres A., Wang M. S., Korbel J. O., Menon R., Chun S.‐M., Kim D., Wilkerson M., Hayes N., Engelmann D., Pützer B., Bos M., Michels S., Vlasic I., Nature 2015, 524, 47. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous