

Neoadjuvant sintilimab plus chemotherapy in EGFR-mutant NSCLC: Phase 2 trial interim results (NEOTIDE/CTONG2104)
- PMID: 38897205
- PMCID: PMC11293361
- DOI: 10.1016/j.xcrm.2024.101615
Neoadjuvant sintilimab plus chemotherapy in EGFR-mutant NSCLC: Phase 2 trial interim results (NEOTIDE/CTONG2104)
Abstract
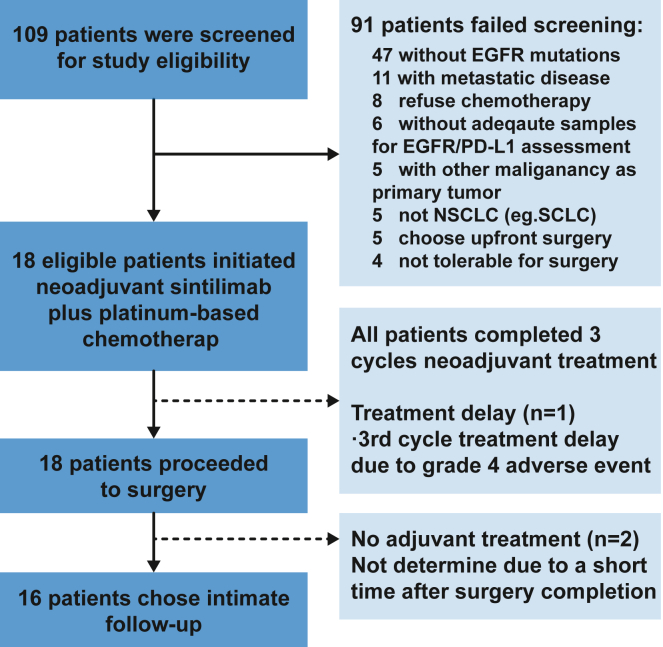
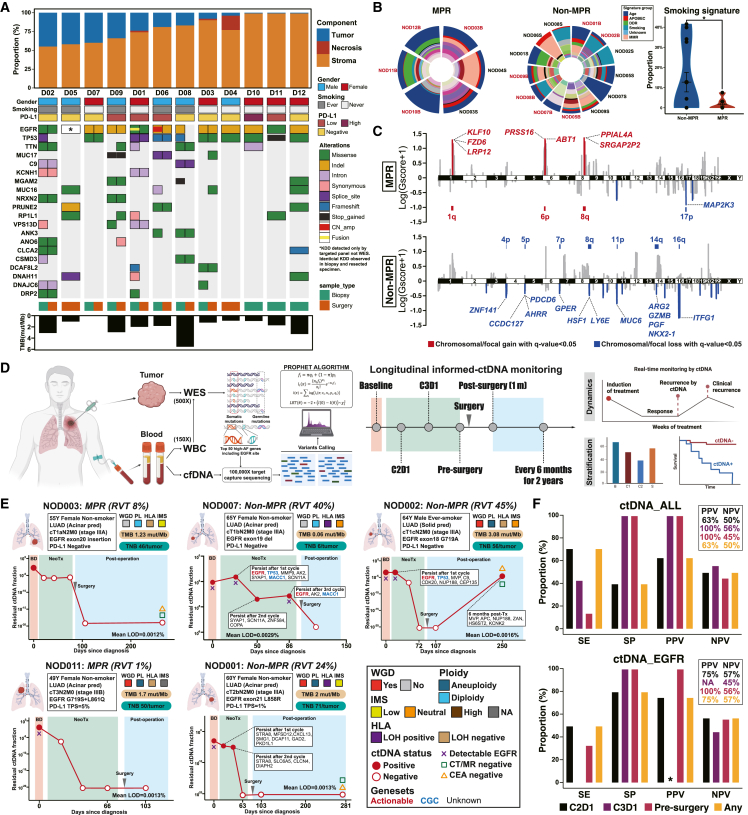
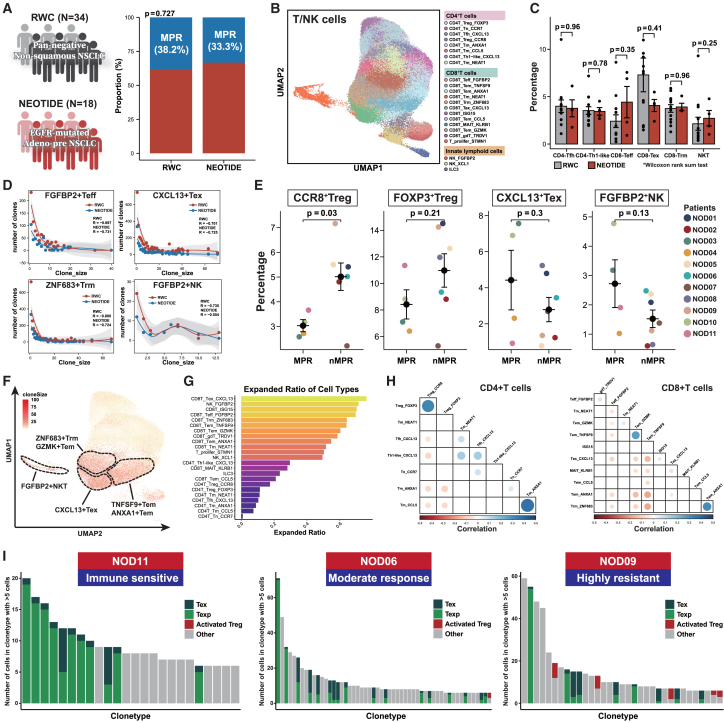
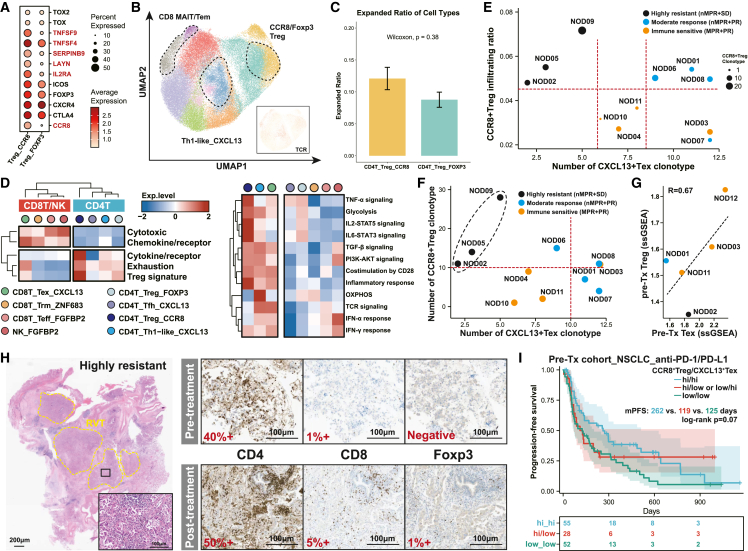
The clinical efficacy of neoadjuvant immunotherapy plus chemotherapy remains elusive in localized epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC). Here, we report interim results of a Simon's two-stage design, phase 2 trial using neoadjuvant sintilimab with carboplatin and nab-paclitaxel in resectable EGFR-mutant NSCLC. All 18 patients undergo radical surgery, with one patient experiencing surgery delay. Fourteen patients exhibit confirmed radiological response, with 44% achieving major pathological response (MPR) and no pathological complete response (pCR). Similar genomic alterations are observed before and after treatment without influencing the efficacy of subsequent EGFR-tyrosine kinase inhibitors (TKIs) in vitro. Infiltration and T cell receptor (TCR) clonal expansion of CCR8+ regulatory T (Treg)hi/CXCL13+ exhausted T (Tex)lo cells define a subtype of EGFR-mutant NSCLC highly resistant to immunotherapy, with the phenotype potentially serving as a promising signature to predict immunotherapy efficacy. Informed circulating tumor DNA (ctDNA) detection in EGFR-mutant NSCLC could help identify patients nonresponsive to neoadjuvant immunochemotherapy. These findings provide supportive data for the utilization of neoadjuvant immunochemotherapy and insight into immune resistance in EGFR-mutant NSCLC.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests W.-Z.Z.. received speech honoraria from AstraZeneca, Roche, Eli Lilly, and Pfizer outside the submitted work. Z.-M.Z. is a founder of Analytical BioSciences. Y.-L.W. received research funding from Roche and speech honoraria from AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi, and he was a research consultant for AstraZeneca. Q.Z. reports honoraria from AstraZeneca, Boehringer Ingelheim, BMS, Eli Lilly, MSD, Pfizer, Roche, and Sanofi outside the submitted work.
Figures



References
-
- Lynch T.J., Bell D.W., Sordella R., Gurubhagavatula S., Okimoto R.A., Brannigan B.W., Harris P.L., Haserlat S.M., Supko J.G., Haluska F.G., et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004;350:2129–2139. doi: 10.1056/NEJMoa040938. - DOI - PubMed
-
- Shi Y., Au J.S.K., Thongprasert S., Srinivasan S., Tsai C.M., Khoa M.T., Heeroma K., Itoh Y., Cornelio G., Yang P.C. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER) J. Thorac. Oncol. 2014;9:154–162. doi: 10.1097/jto.0000000000000033. - DOI - PMC - PubMed
-
- Wu Y.L., Cheng Y., Zhou X., Lee K.H., Nakagawa K., Niho S., Tsuji F., Linke R., Rosell R., Corral J., et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18:1454–1466. doi: 10.1016/s1470-2045(17)30608-3. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
