

Surgical Concepts and Long-term Outcomes of Thalamic Deep Brain Stimulation in Patients with Severe Tourette Syndrome: A Single-center Experience
- PMID: 38897940
- PMCID: PMC11374463
- DOI: 10.2176/jns-nmc.2023-0254
Surgical Concepts and Long-term Outcomes of Thalamic Deep Brain Stimulation in Patients with Severe Tourette Syndrome: A Single-center Experience
Abstract
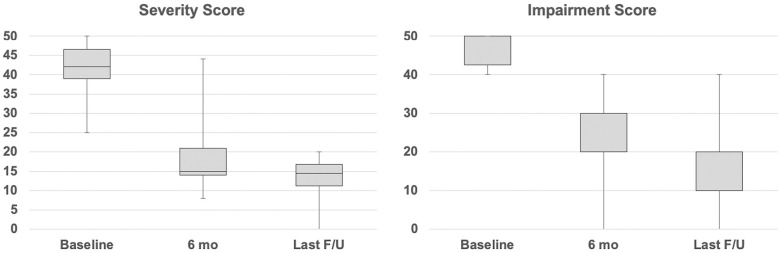
Tourette syndrome (TS) is a developmental neuropsychiatric disorder that is characterized by tic movements. Deep brain stimulation (DBS) may be a treatment option for severe cases refractory to medical and behavioral therapies. In this study, we reviewed the surgical techniques used for DBS in patients with severe TS and its clinical outcomes and sought to determine the optimal surgical procedure and current issues based on our experience and the literature. A total of 14 patients, consisting of 13 men and 1 woman, who underwent centromedian thalamic DBS and were followed up for a mean duration of 2.3 ± 1.0 years, participated in this study. The mean Yale Global Tic Severity Scale severity score significantly improved from 41.4 ± 7.0 at baseline to 19.8 ± 11.4 at 6 months (P = 0.01) and 12.7 ± 6.2 at the last follow-up (P < 0.01). Moreover, the mean Yale Global Tic Severity Scale impairment score significantly improved from 47.1 ± 4.7 at baseline to 23.1 ± 11.1 at 6 months (P < 0.01) and 7.6 ± 2.9 at the last follow-up (P < 0.01). However, there were problems with continuous postoperative monitoring (three cases were lost to follow-up) and surgery-related adverse events, including one case each of lead misplacement and a delayed intracerebral hemorrhage due to severe self-injurious tics. This study aimed to highlight not only the clinical efficacy of DBS for TS but also its challenges. Clinicians should understand the three-dimensional brain anatomy so that they can perform precise surgical procedures, avoid adverse events, and achieve favorable outcomes of DBS for TS.
Keywords: Tourette syndrome; adverse events; deep brain stimulation; microlesion effect; thalamus.
Conflict of interest statement
None.
Figures
References
-
- Dowd RS, Pourfar M, Mogilner AY: Deep brain stimulation for Tourette syndrome: a single-center series. J Neurosurg 128: 596-604, 2018 - PubMed
-
- Baldermann JC, Schüller T, Huys D, et al. : Deep brain stimulation for tourette-syndrome: A systematic review and meta-analysis. Brain Stimul 9: 296-304, 2016 - PubMed
-
- Vandewalle V, van der Linden C, Groenewegen HJ, Caemaert J: Stereotactic treatment of Gilles de la Tourette syndrome by high frequency stimulation of thalamus. Lancet 353: 724, 1999 - PubMed
-
- Hariz MI, Robertson MM: Gilles de la Tourette syndrome and deep brain stimulation. Eur J Neurosci 32: 1128-1134, 2010 - PubMed