

Entrectinib in ROS1-positive advanced non-small cell lung cancer: the phase 2/3 BFAST trial
- PMID: 38898120
- PMCID: PMC11271410
- DOI: 10.1038/s41591-024-03008-4
Entrectinib in ROS1-positive advanced non-small cell lung cancer: the phase 2/3 BFAST trial
Abstract
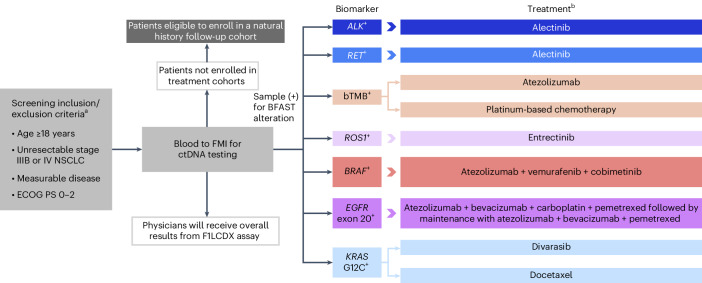
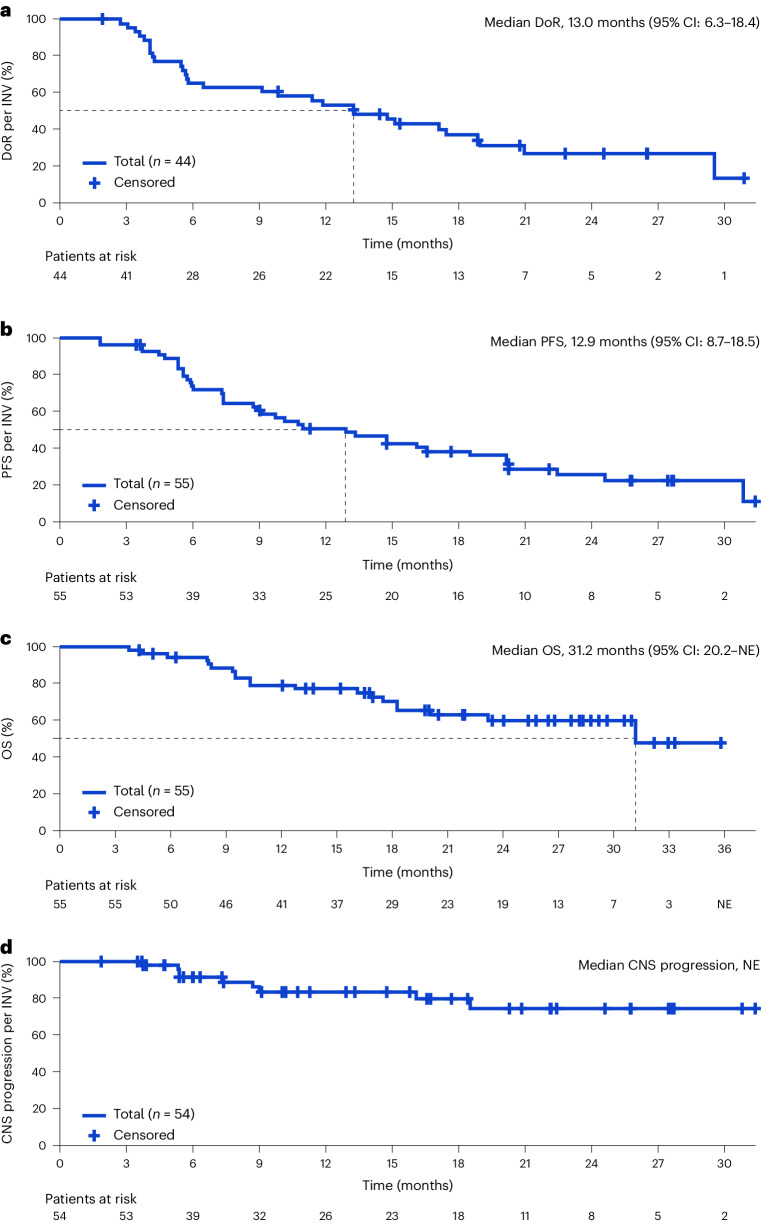
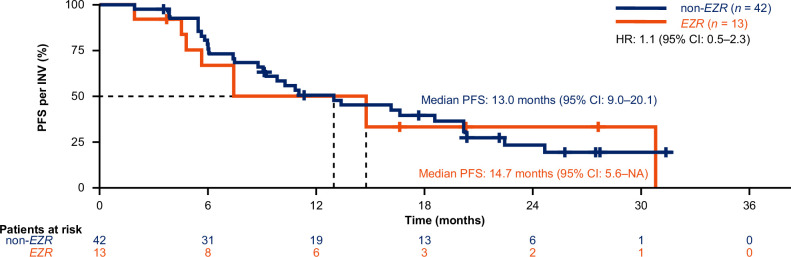
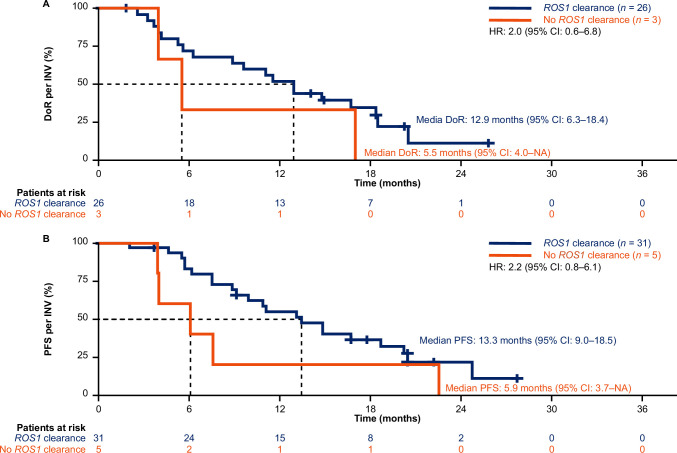
Although comprehensive biomarker testing is recommended for all patients with advanced/metastatic non-small cell lung cancer (NSCLC) before initiation of first-line treatment, tissue availability can limit testing. Genomic testing in liquid biopsies can be utilized to overcome the inherent limitations of tissue sampling and identify the most appropriate biomarker-informed treatment option for patients. The Blood First Assay Screening Trial is a global, open-label, multicohort trial that evaluates the efficacy and safety of multiple therapies in patients with advanced/metastatic NSCLC and targetable alterations identified by liquid biopsy. We present data from Cohort D (ROS1-positive). Patients ≥18 years of age with stage IIIB/IV, ROS1-positive NSCLC detected by liquid biopsies received entrectinib 600 mg daily. At data cutoff (November 2021), 55 patients were enrolled and 54 had measurable disease. Cohort D met its primary endpoint: the confirmed objective response rate (ORR) by investigator was 81.5%, which was consistent with the ORR from the integrated analysis of entrectinib (investigator-assessed ORR, 73.4%; data cutoff May 2019, ≥12 months of follow-up). The safety profile of entrectinib was consistent with previous reports. These results demonstrate consistency with those from the integrated analysis of entrectinib in patients with ROS1-positive NSCLC identified by tissue-based testing, and support the clinical value of liquid biopsies to inform clinical decision-making. The integration of liquid biopsies into clinical practice provides patients with a less invasive diagnostic method than tissue-based testing and has faster turnaround times that may expedite the reaching of clinical decisions in the advanced/metastatic NSCLC setting. ClinicalTrials.gov registration: NCT03178552 .
© 2024. The Author(s).
Conflict of interest statement
S.P. received institutional support for consulting or advising from AbbVie, Amgen, AstraZeneca, Bayer, BeiGene, Biocartis, Boehringer Ingelheim, Bristol Myers Squibb, Clovis, Daiichi Sankyo, Debiopharm, eCancer, Eli Lilly, Elsevier, Foundation Medicine, Illumina, Imedex, IQVIA, Incyte, Janssen, Medscape, Merck Sharp & Dohme, Merck Serono, Merrimack, Novartis, Oncology Education, PharmaMar, Phosplatin Therapeutics, PER, Pfizer, PRIME, Regeneron, RMEI, Roche/Genentech, RTP, Sanofi, Seattle Genetics and Takeda; institutional fees for speaking at company-sponsored public events for AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, eCancer, Eli Lilly, Illumina, Imedex, Medscape, Merck Sharp & Dohme, Novartis, PER, Pfizer, Prime, Roche/Genentech, RTP, Sanofi and Takeda; and institutional grants and research support for the conduct of clinical trials from Amgen, AstraZeneca, Biodesix, Boehringer Ingelheim, Bristol Myers Squibb, Clovis, GlaxoSmithKline, Illumina, Lilly, Merck Sharp & Dohme, Merck Serono, Mirati, Novartis, Pfizer, Phosplatin Therapeutics and Roche/Genentech. S.M.G. received fees for consulting from Roche/Genentech, Takeda, AstraZeneca, Pfizer, Daiichi Sankyo and Eli Lilly; and served on an independent data-monitoring committee for AstraZeneca. T.M. received fees for serving on advisory boards and consulting, and speaker fees and institutional grants and research support, from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pfizer; fees for serving on advisory boards and consulting and speaker fees from ACEA Pharma, Amgen, Boehringer lngelheim Pharmaceuticals, Inc., Daiichi Sankyo, Inc., Fishawack Facilitate, Ltd., Lilly, OrigiMed Co. Ltd. and Sanofi-Aventis; owns stock and has received fees for serving on advisory boards and board of directors/leadership roles from HutchMed; received institutional grants and research support and fees for serving on advisory boards and consulting from Merck Serono and SFJ Pharmaceutical Ltd.; received fees for serving on advisory boards, board of directors/leadership roles and consulting from Lunit, Inc.; received fees for serving on advisory boards and for consulting from AbbVie Inc., BerryOncology, Blueprint Medicines Corporation, C4 Therapeutics, Inc, CStone Pharmaceuticals, Curio Science, Eisai, Gilead Sciences, Inc., Gritstone Oncology, Inc., Guardant Health, Hengrui Therapeutics, Inc., IQVIA, Janssen, lgnyta, Inc., lncyte Corporation, lnivata, Loxo Oncology Inc., Mirati Therapeutics, Inc., Puma Biotechnology, Inc., Vertex Pharmaceuticals and Yuhan Corporation; received speaker fees and fees for consulting from Alpha Biopharma Co., Ltd., Amoy Diagnostics Co., Ltd., AstraZeneca (before 1 January 2019) and BeiGene; received fees for serving on advisory boards and institutional grants and research support from AstraZeneca, Gl Therapeutics, Inc. and Takeda; received institutional grants and research support from Roche and XCovery; received speaker fees from Daz Group, InMed Medical Communication, Janssen Pharmaceutica NV, Liangyihui Network Technology Co., Ltd., Lucence Health, Inc., MD Health Brazil, Medscape LLC, Merck Pharmaceuticals HK Ltd., P. Permanyer SL, PeerVoice, Physicians’ Education Resource, PrIME Oncology, Research to Practice, Roche Pharmaceuticals/Diagnostic/Foundation MedicineOne, Shanghai BeBirds Translation and Consulting Co., Ltd., Taiho, Takeda Oncology and touchIME; received fees for consulting from Elevation Oncology, MoreHealth, Qiming Development (HK) Ltd., Roche Pharmaceuticals and Takeda Pharmaceuticals HK Ltd.; received fees for serving on advisory boards for Roche/Genentech and Virtus Medical Group; received fees for a board of directors/leadership role with AstraZeneca PLC; discloses serving on advisory boards (uncompensated) for geneDecode Co., Ltd.; owns stock from Act Genomics-Sanomics Group and Aurora Tele-Oncology Ltd.; and declares uncompensated board of directors/leadership roles with the American Society of Clinical Oncology, Asian Thoracic Oncology Research Group, Chinese Lung Cancer Research Foundation Limited, Chinese Society of Clinical Oncology, Hong Kong Cancer Fund, Hong Kong Cancer Therapy Society, International Association for the Study of Lung Cancer (ending 30 April 2019) and St. Stephen’s College & Preparatory School. E.N. received research grant support from Pfizer, F. Hoffmann-La Roche Ltd, Bristol Myers Squibb and Merck Serono and participated in advisory boards or gave lectures for Bristol Myers Squibb, Merck Sharp & Dohme, Lilly, F. Hoffmann-La Roche Ltd, Pfizer, Takeda, Boehringer Ingelheim, Amgen, Merck Serono, Sanofi, Bayer, Janssen, Pierre Fabre, Qiagen, Apollomics, Daichi Sankyo and AstraZeneca. S.K. has nothing to declare. A.S. received advisory/consultancy/speaker fees from AMGEN, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Inc., Ipsen, Janssen, Lilly, MSD, Pfizer, F. Hoffmann-La Roche Ltd, Sanofi and Takeda. J.C. received advisory/consultancy/speaker fees from AbbVie, AMGEN, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Inc., Merck Sharp & Dohme, Lilly, Novartis, Pfizer, F. Hoffmann-La Roche Ltd, Sanofi and Takeda. S.S. received research grant support from AnHeart, AstraZeneca, Chugai Pharmaceutical, MSD, Daiichi Sankyo, Bristol Myers Squibb, Nippon Boehringer Ingelheim, Ono Pharmaceutical, AbbVie, Amgen, Taiho Pharmaceutical, Takeda and Clinipace; and honoraria from AstraZeneca, Chugai Pharmaceutical, Ono Pharmaceutical, Bristol Myers Squibb, MSD, Nippon Boehringer Ingelheim, Pfizer, Taiho Pharmaceutical, Eli Lilly, Novartis, Kyowa Kirin, Takeda, Nippon Kayaku, Merck, Amgen, AbbVie, Otsuka, Thermo Fisher Scientific and Towa Pharmaceutical. C.-H.C. received honoraria from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai Pharmaceutical, Eli Lilly, Janssen, Merck KGaA, MSD, Novartis, Ono Pharmaceutical, Pfizer, F. Hoffmann-La Roche and Takeda. C.-J.Y. has nothing to declare. M. Moskovitz received honoraria from Roche Israel, BMS, Astra Zeneca, Takeda, Novartis, MSD, Pfizer and Merck; had an advisory role for Amgen, Bayer, Pfizer and Takeda; and received a research grant from Astra Zeneca. T.T. declares full-time employment at Chugai Pharmaceutical Co., Ltd., which is an F. Hoffmann-La Roche Ltd. company; and stocks/shares in Chugai Pharmaceutical Co., Ltd. R.N. declares full-time employment at, and stocks/shares in, Genentech. S.M.S. declares full-time employment at Genentech, and stocks/shares in F. Hoffmann-La Roche Ltd. M. Maclennan declares employment at Syneos Health and work as a Study Statistician in FSP model for F. Hoffmann-La Roche Ltd on a full-time basis. M. Mathisen, V.B.-P., C.D. and Z.J.A. declare full-time employment at, and stocks/shares in, Genentech. V.A. declares full-time employment at, and stocks/shares in, F. Hoffmann-La Roche Ltd. R.D. declares advisory/consultancy fees from F. Hoffmann-La Roche Ltd, Foundation Medicine, Pfizer, AstraZeneca, Novartis, Merck Sharp & Dohme, Karyopharm and Takeda; honoraria from F. Hoffmann-La Roche Ltd, AstraZeneca and Amgen; and participated in Data Safety Monitoring Boards/advisory boards for F. Hoffmann-La Roche, Ltd, AstraZeneca, Amgen, Pfizer and Merck Sharp & Dohme.
Figures
References
-
- NCCN Clinical Practice Guidelines in Oncology for Non-Small Cell Lung Cancer v.1.2024 (National Comprehensive Cancer Network, 2024). - PubMed
-
- Robert, N. J. et al. Biomarker tissue journey among patients (pts) with untreated metastatic non-small cell lung cancer (mNSCLC) in the U.S. Oncology Network community practices. J. Clin. Oncol.39, 9004 (2021).10.1200/JCO.2021.39.15_suppl.9004 - DOI
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
