

Functional outcomes and quality of life following open versus laparoscopic versus robot-assisted versus transanal total mesorectal excision in rectal cancer patients: a systematic review and meta-analysis
- PMID: 38898341
- PMCID: PMC11289076
- DOI: 10.1007/s00464-024-10934-4
Functional outcomes and quality of life following open versus laparoscopic versus robot-assisted versus transanal total mesorectal excision in rectal cancer patients: a systematic review and meta-analysis
Abstract
Background: The standard surgical treatment for rectal cancer is total mesorectal excision (TME), which may negatively affect patients' functional outcomes and quality of life (QoL). However, it is unclear how different TME techniques may impact patients' functional outcomes and QoL. This systematic review and meta-analysis evaluated functional outcomes of urinary, sexual, and fecal functioning as well as QoL after open, laparoscopic (L-TME), robot-assisted (R-TME), and transanal total mesorectal excision (TaTME).
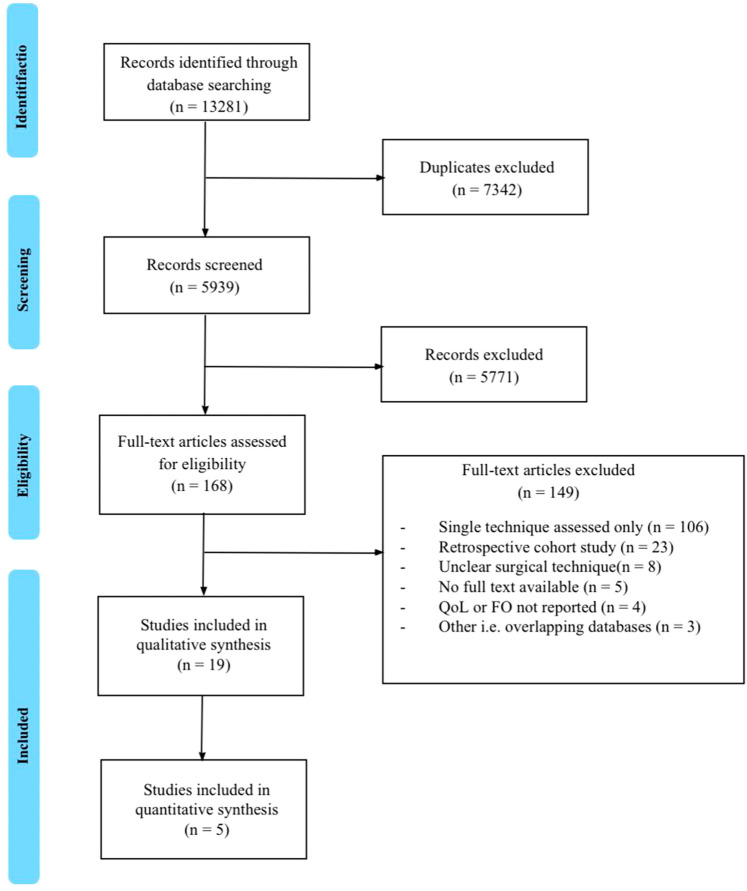
Methods: A systematic review and meta-analysis, based on the preferred reporting items for systematic reviews and meta-analysis statement, were conducted (PROSPERO: CRD42021240851). A literature review was performed (sources: PubMed, Medline, Embase, Scopus, Web of Science, and Cochrane Library databases; end-of-search date: September 1, 2023), and a quality assessment was performed using the Methodological index for non-randomized studies. A random-effects model was used to pool the data for the meta-analyses.
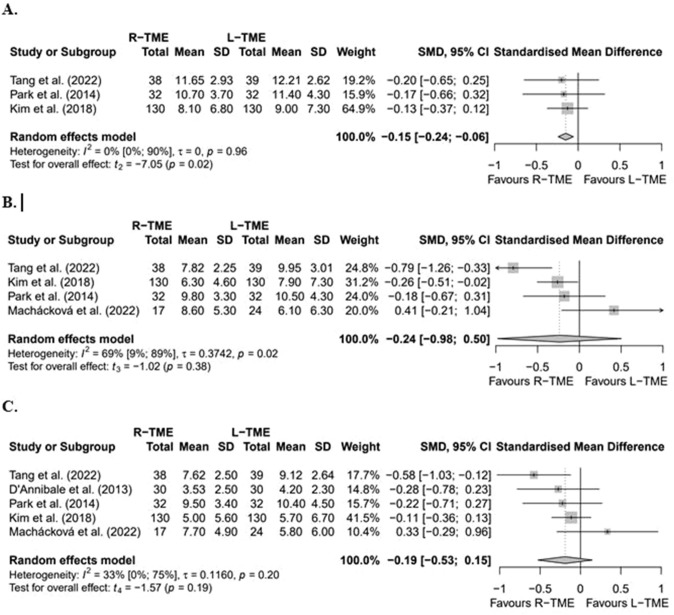
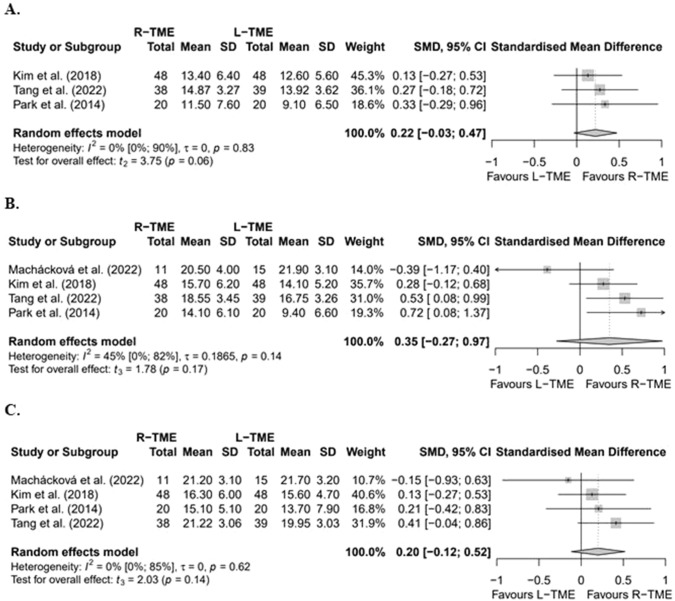
Results: Nineteen studies were included, reporting on 2495 patients (88 open, 1171 L-TME, 995 R-TME, and 241 TaTME). Quantitative analyses comparing L-TME vs. R-TME showed no significant differences regarding urinary and sexual functioning, except for urinary function at three months post-surgery, which favoured R-TME (SMD [CI] -0 .15 [- 0.24 to - 0.06], p = 0.02; n = 401). Qualitative analyses identified most studies did not find significant differences in urinary, sexual, and fecal functioning and QoL between different techniques.
Conclusions: This systematic review and meta-analysis highlight a significant gap in the literature concerning the evaluation of functional outcomes and QoL after TME for rectal cancer treatment. This study emphasizes the need for high-quality, randomized-controlled, and prospective cohort studies evaluating these outcomes. Based on the limited available evidence, this systematic review and meta-analysis suggests no significant differences in patients' urinary, sexual, and fecal functioning and their QoL across various TME techniques.
Keywords: Functional outcomes; Meta-analysis; Quality of life; Rectal cancer; Systematic review; Total mesorectal excision.
© 2024. The Author(s).
Conflict of interest statement
Esther Consten is a proctor for Intuitive Surgical and received a grant from this organization for the Vantage trial. No (financial) support from this organization has been received for the submitted manuscript. Neither have there been any other activities or relations that have influenced the submitted work. Drs. Ritch Geitenbeek, Thijs Burghgraef, Carmen Moes, Roel Hompes, and Adelita Ranchor have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Rubinkiewicz M, Zarzycki P, Witowski J, Pisarska M, Gajewska N, Torbicz G, Nowakowski M, Major P, Budzyński A, Pȩdziwiatr M (2019) Functional outcomes after resections for low rectal tumors: comparison of transanal with laparoscopic total mesorectal excision. BMC Surg. 10.1186/S12893-019-0550-4 10.1186/S12893-019-0550-4 - DOI - PMC - PubMed
-
- Campelo P, Barbosa E (2016) Functional outcome and quality of life following treatment for rectal cancer. J Coloproctol 36:251–261 10.1016/j.jcol.2016.05.001 - DOI
-
- Veltcamp Helbach M, Koedam TWA, Knol JJ, Velthuis S, Bonjer HJ, Tuynman JB, Sietses C (2019) Quality of life after rectal cancer surgery: differences between laparoscopic and transanal total mesorectal excision. Surg Endosc 33:79–87. 10.1007/s00464-018-6276-z 10.1007/s00464-018-6276-z - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
