

Creatinine, cystatin C, muscle mass, and mortality: Findings from a primary and replication population-based cohort
- PMID: 38898741
- PMCID: PMC11294032
- DOI: 10.1002/jcsm.13511
Creatinine, cystatin C, muscle mass, and mortality: Findings from a primary and replication population-based cohort
Abstract
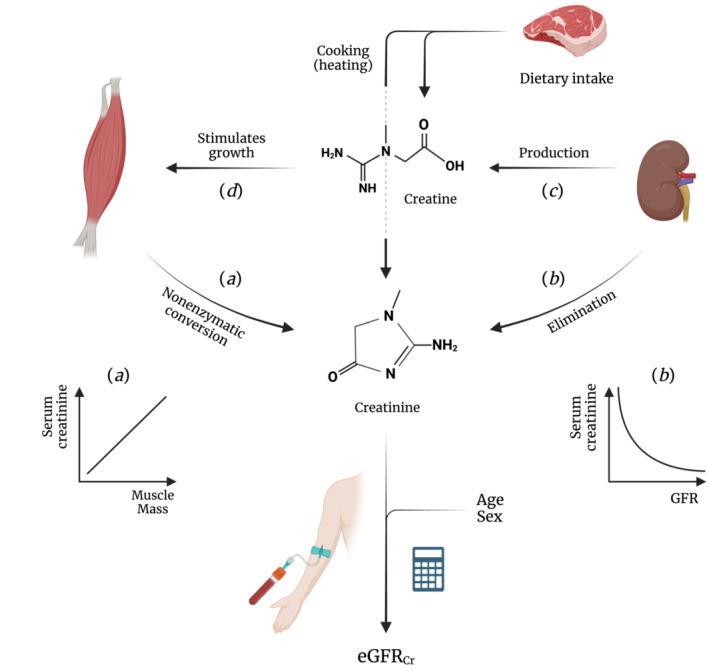
Background: Serum creatinine is used as initial test to derive eGFR and confirmatory testing with serum cystatin C is recommended when creatinine-based eGFR is considered less accurate due to deviant muscle mass. Low muscle mass is associated with increased risk of premature mortality. However, the associations of serum creatinine and cystatin C with muscle mass and mortality remain unclear and require further investigation to better inform clinical decision-making.
Methods: We included 8437 community-dwelling adults enrolled in the Dutch PREVEND study and 5033 in the US NHANES replication cohort. Associations of serum creatinine and/or cystatin C with muscle mass surrogates and mortality were quantified with linear and Cox proportional hazards regression, respectively. Missing observations in covariates were multiply imputed using Substantive Model Compatible Fully Conditional Specification.
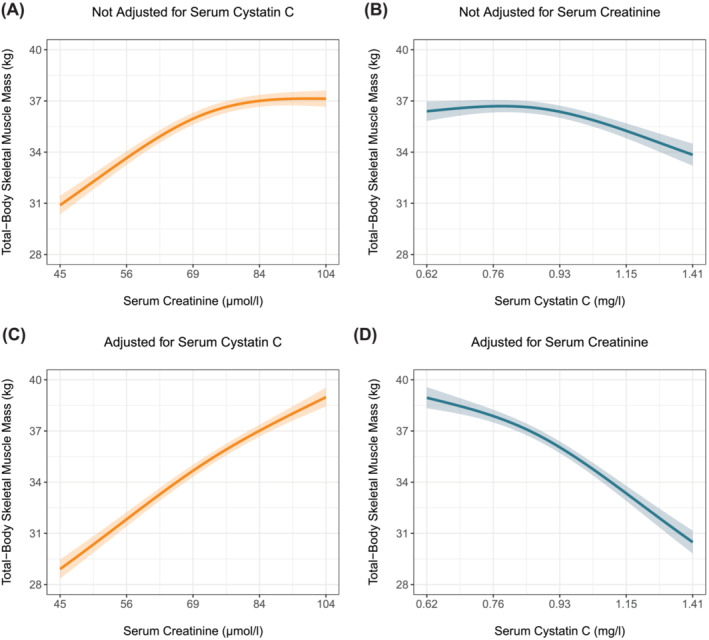
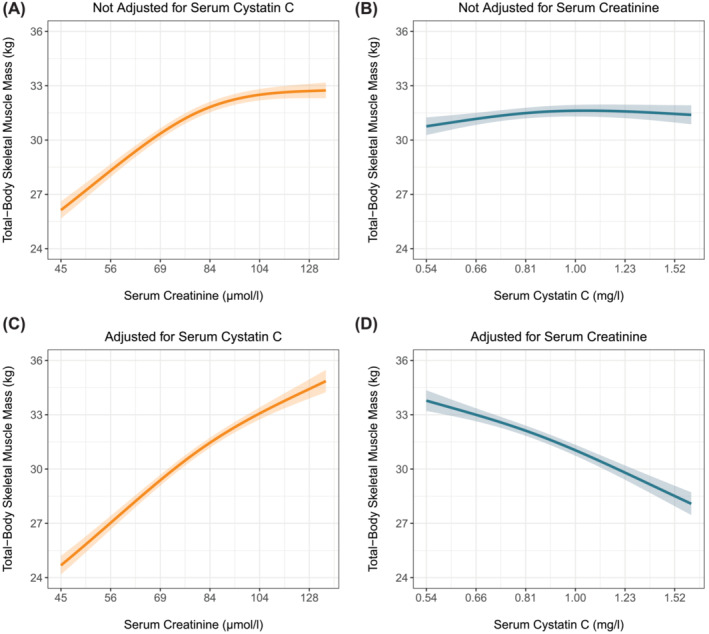
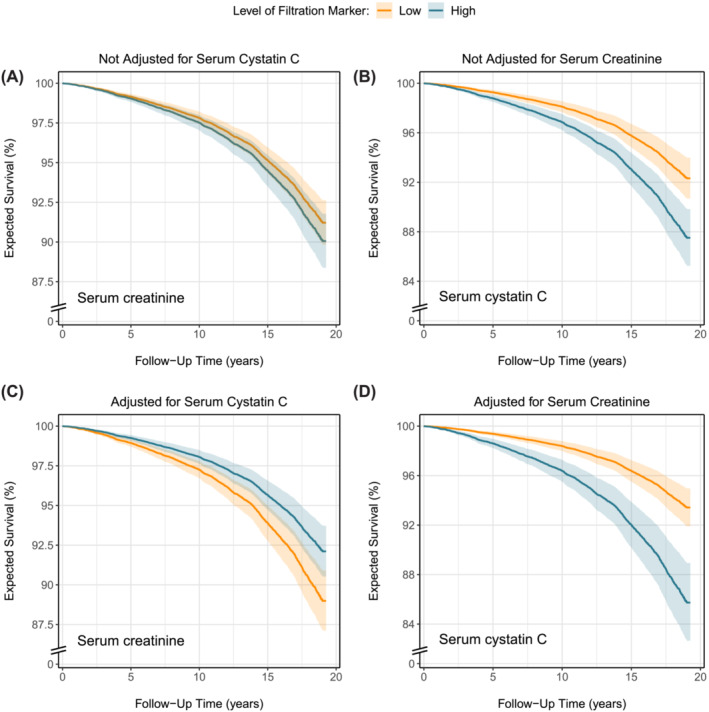
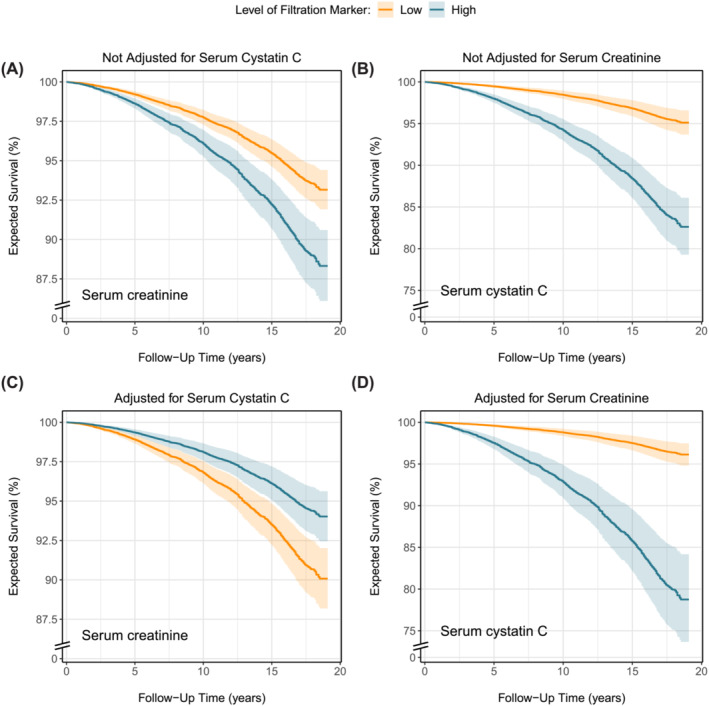
Results: Mean (SD) age of PREVEND and NHANES participants (50% and 48% male) were 49.8 (12.6) and 48.7 (18.7) years, respectively. Median (Q1-Q3) serum creatinine and cystatin C were 71 (61-80) and 80 (62-88) μmol/L and 0.87 (0.78-0.98) and 0.91 (0.80-1.10) mg/L, respectively. Higher serum creatinine was associated with greater muscle mass, while serum cystatin C was not associated with muscle mass. Adjusting both markers for each other strengthened the positive relationship between serum creatinine and muscle mass and revealed an inverse association between serum cystatin C and muscle mass. In the PREVEND cohort, 1636 (19%) deaths were registered over a median follow-up of 12.9 (5.8-16.3) years with a 10-year mortality rate (95% CI) of 7.6% (7.1-8.2%). In the NHANES, 1273 (25%) deaths were registered over a median follow-up of 17.9 (17.3-18.5) years with a 10-year mortality rate of 13.8% (12.8-14.7%). Both markers were associated with increased mortality. Notably, when adjusted for each other, higher serum creatinine was associated with decreased mortality, while the association between serum cystatin C and increased mortality strengthened. The shapes of the associations in the PREVEND study and NHANES were almost identical.
Conclusions: The strong association between serum creatinine and muscle mass challenges its reliability as GFR marker, necessitating a more cautious approach in its clinical use. The minimal association between serum cystatin C and muscle mass supports its increased use as a more reliable alternative in routine clinical practice.
Keywords: Creatinine; Cystatin C; General population; Kidney function; Mortality; Muscle mass.
© 2024 The Author(s). Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO . Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2012;2013:1–150.
-
- Heymsfield SB, Arteaga C, Mcmanus C, Smith J, Moffltt S. Perspective in nutrition measurement of muscle mass in humans: validity of the 24‐hour urinary creatinine method. Am J Clin Nutr 1983;37:478–494. - PubMed
-
- Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function‐measured and estimated glomerular filtration rate. N Engl J Med 2006;354:2473–2483. - PubMed
-
- Wang XH, Mitch WE, Price SR. Pathophysiological mechanisms leading to muscle loss in chronic kidney disease. Nat Rev Nephrol 2022;18:138–152. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
