

Leptomeningeal enhancement in multiple sclerosis: a focus on patients treated with hematopoietic stem cell transplantation
- PMID: 38899059
- PMCID: PMC11186296
- DOI: 10.3389/fneur.2024.1373385
Leptomeningeal enhancement in multiple sclerosis: a focus on patients treated with hematopoietic stem cell transplantation
Abstract
Background: Leptomeningeal enhancement (LME) is considered an MRI marker of leptomeningeal inflammation in inflammatory neurological disorders, including multiple sclerosis (MS). To our knowledge, no disease-modifying therapies (DMTs) have been demonstrated to affect LME number or morphology so far.
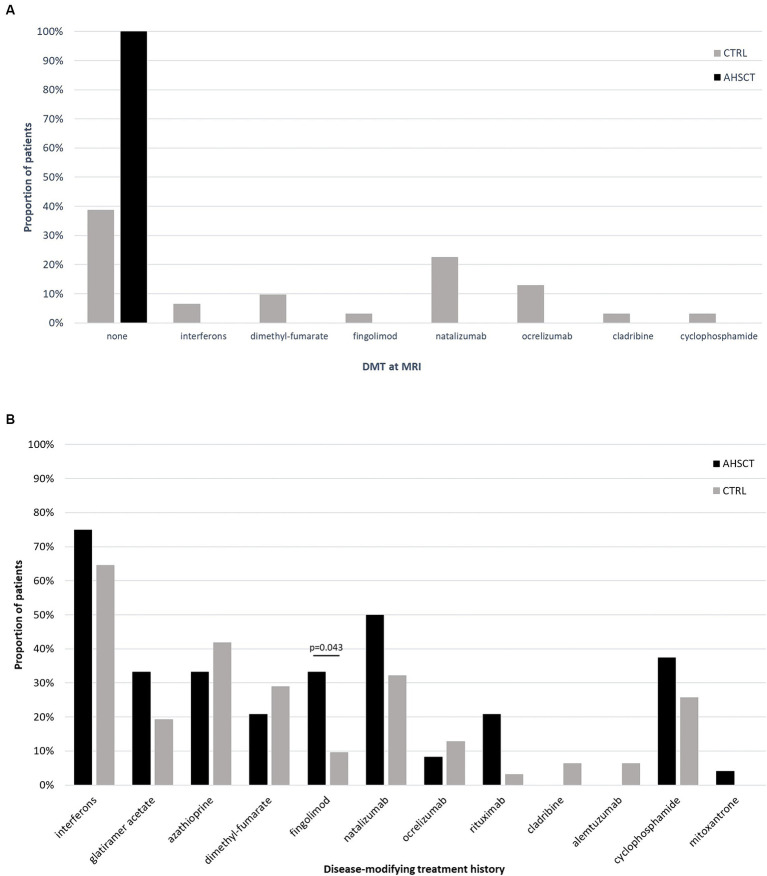
Methods: Monocentric study investigating the frequency and number of LME in a cohort of people with (pw)MS who performed a 3 T brain MRI with a standardized protocol (including a post-contrast FLAIR sequence), and exploring the impact of autologous hematopoietic stem cell transplantation (AHSCT) on this marker. In a longitudinal pilot study, consecutive MRIs were also analyzed in a subgroup of pwMS, including patients evaluated both pre- and post-AHSCT.
Results: Fifty-five pwMS were included: 24/55 (44%) had received AHSCT (AHSCT group) and 31 other treatments (CTRL group). At least one LME was identified in 19/55 (35%) cases (42 and 29% in the AHSCT and CTRL groups, respectively; p = 0.405). In the AHSCT group, LME number correlated with age at AHSCT (R = 0.50; p = 0.014), but not with age at post-treatment MRI. In the longitudinal pilot study (n = 8), one LME disappeared following AHSCT in 1/4 patients, whereas LME number was unchanged in the remaining four pwMS from the CTRL group.
Discussion: These results suggest that AHSCT may affect development and persistence of LME, strengthening the indication for early use of effective therapies bioavailable within the central nervous system (CNS), and therefore potentially targeting compartmentalized inflammation.
Keywords: autologous hematopoietic stem cell transplantation; biomarker; chronic inflammation; leptomeningeal enhancement; magnetic resonance imaging; multiple sclerosis; transplant.
Copyright © 2024 Marchi, Mariottini, Viti, Bianchi, Nozzoli, Repice, Boncompagni, Ginestroni, Damato, Barilaro, Chiti, Saccardi, Fainardi and Massacesi.
Conflict of interest statement
AM reports personal fees from Sanofi, Janssen, Biogen, and Novartis; non-financial support from Biogen, Novartis, and Sanofi, outside the submitted work. RS reports consulting fees from Sanofi and Therakos. LuM reports non-financial support from Biogen, Novartis, Merck Serono, Genzyme, and Teva, outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources