

Metabolic Acidosis Is Associated With an Accelerated Decline of Allograft Function in Pediatric Kidney Transplantation
- PMID: 38899185
- PMCID: PMC11184248
- DOI: 10.1016/j.ekir.2024.04.007
Metabolic Acidosis Is Associated With an Accelerated Decline of Allograft Function in Pediatric Kidney Transplantation
Abstract
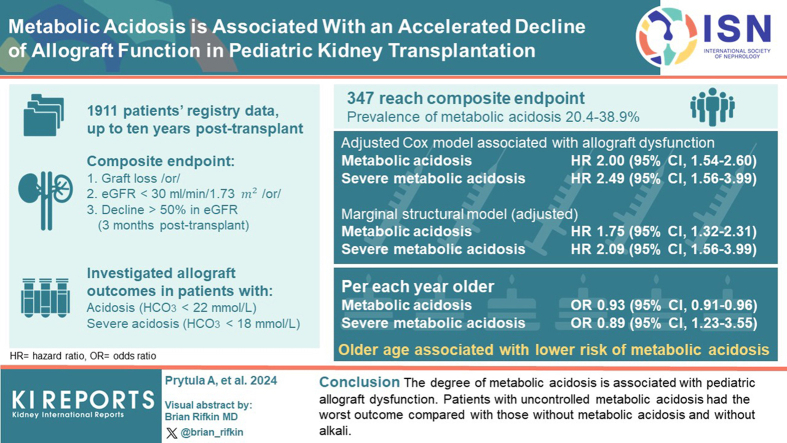
Introduction: We investigated the relationship between metabolic acidosis over time and allograft outcome in pediatric kidney transplantation (KTx).
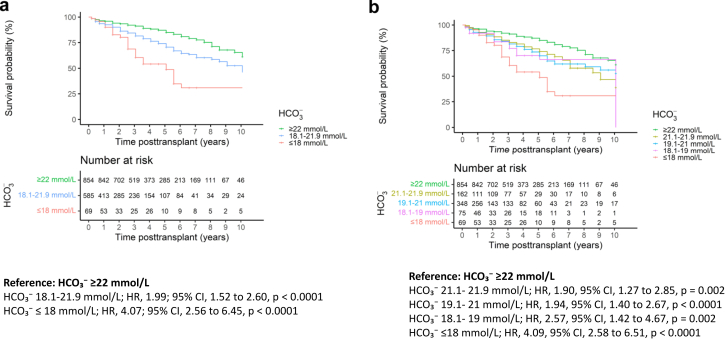
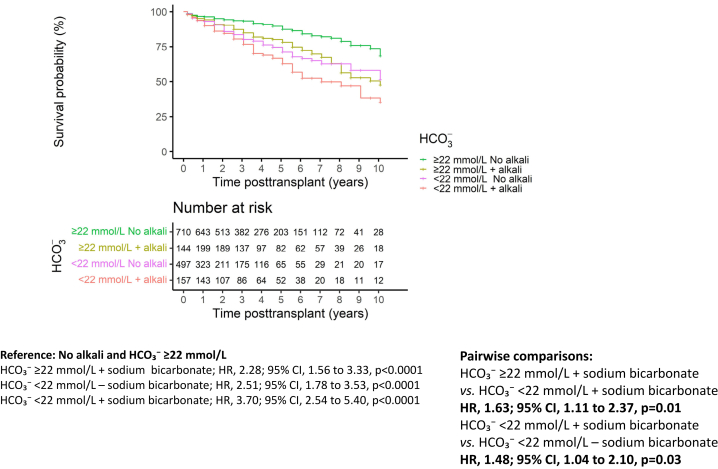
Methods: This registry study collected data up to 10 years posttransplant. Survival analysis for a composite end point of graft loss or estimated glomerular filtration rate (eGFR) ≤ 30 ml/min per 1.73 m2 or ≥50% decline from eGFR at month 3 posttransplant was performed. The association of serum bicarbonate concentration (HCO3 -) < 22 mmol/l (metabolic acidosis) and HCO3 - < 18 mmol/l (severe metabolic acidosis) with allograft outcome was investigated using stratified Cox models and marginal structural models. Secondary analyses included the identification of risk factors for metabolic acidosis and the relationship between alkali supplementation and allograft outcome.
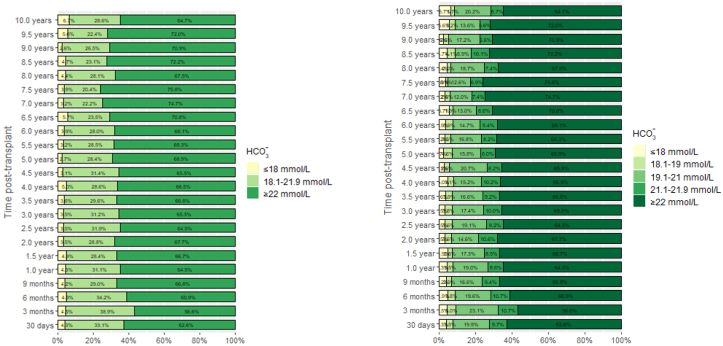
Results: We report on 1911 patients, of whom 347 reached the composite end point. The prevalence of metabolic acidosis over time ranged from 20.4% to 38.9%. In the adjusted Cox models, metabolic acidosis (hazard ratio [HR], 2.00; 95% confidence interval [CI], 1.54-2.60) and severe metabolic acidosis (HR, 2.49; 95% CI, 1.56-3.99) were associated with allograft dysfunction. Marginal structural models showed similar results (HR, 1.75; 95% CI, 1.32-2.31 and HR, 2.09; 95% CI, 1.23-3.55, respectively). Older age was associated with a lower risk of metabolic acidosis (odds ratio [OR] 0.93/yr older; 95% CI, 0.91-0.96) and severe metabolic acidosis (OR, 0.89; 95% CI, 0.84-0.95). Patients with uncontrolled metabolic acidosis had the worst outcome compared to those without metabolic acidosis and without alkali (HR, 3.70; 95% CI, 2.54-5.40).
Conclusion: The degree of metabolic acidosis is associated with allograft dysfunction.
Keywords: acidosis; pediatric; transplantation.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
