

Polyomavirus Nephropathy in ABO Blood Group-Incompatible Kidney Transplantation: Torque Teno Virus and Immunosuppressive Burden as an Approximation to the Problem
- PMID: 38899213
- PMCID: PMC11184242
- DOI: 10.1016/j.ekir.2024.04.003
Polyomavirus Nephropathy in ABO Blood Group-Incompatible Kidney Transplantation: Torque Teno Virus and Immunosuppressive Burden as an Approximation to the Problem
Abstract
Introduction: Earlier reports suggest that patients after ABO-incompatible kidney transplantation (ABOi) are at enhanced risk of developing BK-virus (BKV, also known as BK polyomavirus [BKPyV]) nephropathy (BKPyVAN). It remains elusive whether this is a result of more intense immunosuppression or an ABOi-associated "intrinsic attribute." To address this question, we measured Torque Teno virus (TTV) loads as a quantitative proxy for immunosuppressive depth in ABOi recipients and compared them to human leukocyte antigen-incompatible (HLAi, i.e. pretransplant donor-specific antibody-positive) and standard-risk transplant recipients.
Methods: Our retrospective study screened 2256 consecutive kidney transplantations performed between 2007 and 2020 at the Medical University of Vienna. Out of 629 in-principle eligible transplantations, we were able to include 465 patients: 42 ABOi, 106 HLAi, and 317 control recipients. Longitudinal TTV- polymerase chain reaction (PCR) and BKV-PCR was carried out at predefined timepoints and ranged from pretransplant until month 24 posttransplantation. TTV loads and immunosuppression were evaluated in the context of BKV-associated complications.
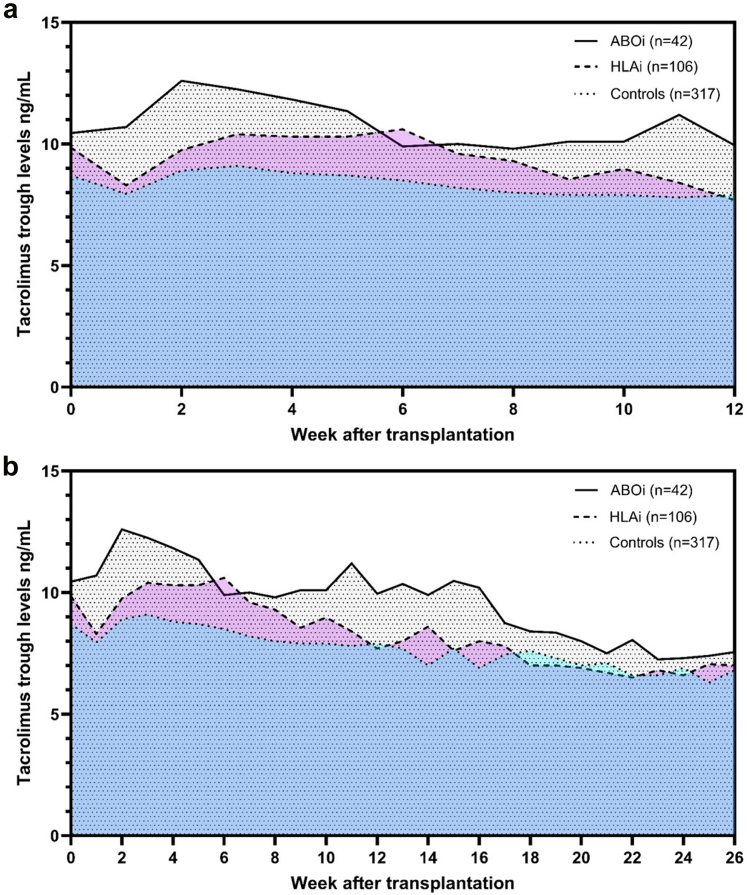
Results: ABOi recipients had a higher TTV load compared to HLAi and controls both at month 3 (median 1.5 × 109 vs. 2.4 × 108 vs. 9.1 × 107; P = 0.010) and at month 6 (3.1 × 109 vs. 1.4 × 107 vs. 6.4 × 107; P = 0.014) posttransplantation. Tacrolimus exposure was significantly higher in ABOi patients compared to HLAi and control patients (ABOi vs. HLAi: P = 0.007; ABOi vs. controls: P < 0.0001). Biopsy-proven BKPyVAN was more frequent in ABOi recipients when compared to HLAi and control recipients (11.9% vs. 2.8% vs. 4.1%; P = 0.046).
Conclusion: Our data support the assumption that ABOi patients are indeed at higher risk to develop BKPyVAN. A higher TTV load and immunosuppressive burden suggest that intense immunosuppression, rather than an "intrinsic attribute" conferred by ABOi, may contribute to this finding.
Keywords: ABOi transplantation; BK-virus nephropathy; Torque Teno virus; kidney transplantation.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures






References
LinkOut - more resources
Full Text Sources
