

The Effect of Randomized Beta-Carotene Supplementation on CKD in Men
- PMID: 38899218
- PMCID: PMC11184243
- DOI: 10.1016/j.ekir.2024.04.001
The Effect of Randomized Beta-Carotene Supplementation on CKD in Men
Abstract
Introduction: Beta-carotene (BC) protects the body against free radicals that may damage the kidney and lead to the development of acute kidney injury and chronic kidney disease (CKD). Previous studies in animal models have demonstrated a potential protective effect of 30 mg/kg BC supplementation on renal ischemia or reperfusion injury and subsequently improved kidney function. The extension of these findings to humans, however, remains unclear.
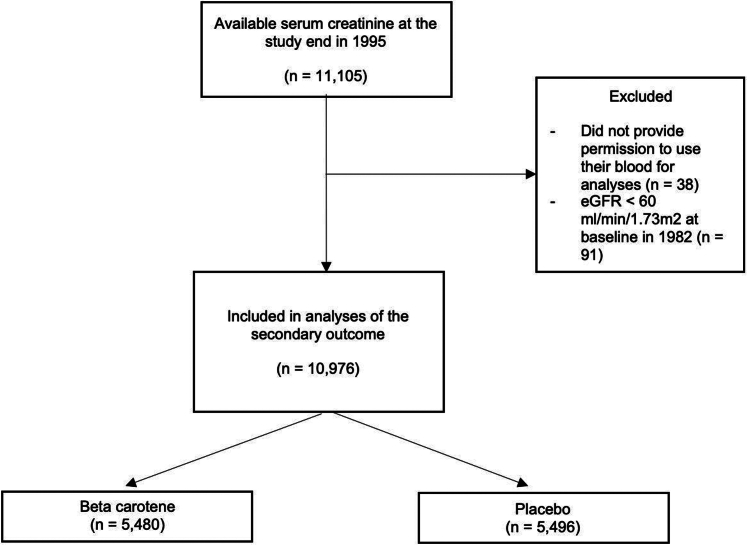
Methods: Our study leverages previously collected data from the Physicians' Health Study I (PHS I), a large-scale, long-term, randomized trial of middle-aged and older US male physicians testing 50 mg BC every other day for primary prevention of cardiovascular disease and cancer. We examined the impact of randomized BC supplementation on self-reported incident CKD identified by self-reports stating "yes" to kidney disease from annual follow-up questionnaires from randomization in 1982 through the end of the randomized BC intervention at the end of 1995, and on CKD defined as an estimated glomerular filtration rate (eGFR) < 60 ml/min per 1.73 m2 at the end of 1995. Analyses compared incident CKD between BC supplementation and placebo using Cox proportional hazards regression models and logistic regression. We also examined whether smoking status (current vs. former or never smoker) or other factors modified the effect of randomized BC supplementation on CKD.
Results: A total of 10,966 participants were randomized to BC, and 10,952 participants were randomized to a placebo group. Baseline characteristics between randomized BC groups were similar. There was no significant benefit between BC supplementation and self-reported incident CKD after adjusting for age and randomized aspirin treatment (hazard ratio [HR] = 0.97, 95% confidence interval [CI]: 0.86-1.08, P-value = 0.56). Stratified by smoking status, there was no significant benefit of BC supplementation and self-reported incident CKD either among former or never smokers (HR = 0.95, 95% CI: 0.84-1.07, P-value = 0.41) or current smokers (HR = 1.08, 95% CI: 0.78-1.50, P-value = 0.64). Smoking status did not modify the association between BC supplementation and incident CKD (P-interaction = 0.47). In subgroup analysis among those with available serum creatinine at the study end (5480 with BC and 5496 with placebo), there was no significant benefit between BC supplementation and CKD based on eGFR < 60 ml/min per 1.73 m2 (odds ratio [OR] = 0.96, 95% CI: 0.85-1.08, P-value = 0.49).
Conclusion: Long-term randomized BC supplementation did not affect the risk of incident CKD in middle-aged and older male physicians.
Keywords: beta-carotene; kidney disease; randomized controlled trials.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures


Similar articles
-
Association of smoking with incident CKD risk in the general population: A community-based cohort study.PLoS One. 2020 Aug 27;15(8):e0238111. doi: 10.1371/journal.pone.0238111. eCollection 2020. PLoS One. 2020. PMID: 32853266 Free PMC article.
-
β-Carotene Supplementation and Lung Cancer Incidence in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study: The Role of Tar and Nicotine.Nicotine Tob Res. 2019 Jul 17;21(8):1045-1050. doi: 10.1093/ntr/nty115. Nicotine Tob Res. 2019. PMID: 29889248 Free PMC article. Clinical Trial.
-
Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project.Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
-
Design of Physicians' Health Study II--a randomized trial of beta-carotene, vitamins E and C, and multivitamins, in prevention of cancer, cardiovascular disease, and eye disease, and review of results of completed trials.Ann Epidemiol. 2000 Feb;10(2):125-34. doi: 10.1016/s1047-2797(99)00042-3. Ann Epidemiol. 2000. PMID: 10691066 Review.
-
Association between Monocyte Count and Risk of Incident CKD and Progression to ESRD.Clin J Am Soc Nephrol. 2017 Apr 3;12(4):603-613. doi: 10.2215/CJN.09710916. Epub 2017 Mar 27. Clin J Am Soc Nephrol. 2017. PMID: 28348030 Free PMC article.
References
-
- Centers for Disease Control and Prevention . US Department of Health and Human Services, Centers for Disease Control and Prevention; 2021. Chronic Kidney Disease in the United States, 2021.https://nccd.cdc.gov/CKD/Documents/Chronic-Kidney-Disease-in-the-US-2021...
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
