

Pelvic Floor Rehabilitation After Rectal Cancer Surgery One-year follow-up of a Multicenter Randomized Clinical Trial (FORCE trial)
- PMID: 38899475
- PMCID: PMC11723484
- DOI: 10.1097/SLA.0000000000006402
Pelvic Floor Rehabilitation After Rectal Cancer Surgery One-year follow-up of a Multicenter Randomized Clinical Trial (FORCE trial)
Abstract
Objective: This study aims to evaluate the effects of pelvic floor rehabilitation (PFR) after low anterior resection (LAR) at one-year follow-up.
Summary background data: After LAR, with restoration of bowel continuity, up to 90% of patients develop anorectal dysfunction, significantly impacting their quality of life. However, standardized treatment is currently unavailable. The FORCE trial demonstrated the beneficial effects of PFR after three months regarding specific domains of the Fecal Incontinence QoL (FIQL) questionnaire and urgency compared to usual care.
Methods: The FORCE trial is a multicenter, two-arm, randomized clinical trial. All patients undergoing LAR were randomly assigned to receive either usual care or a standardized PFR program. The primary outcome measure is the Wexner incontinence score, and the secondary endpoints included the LARS score, the EORTC colorectal-specific QoL questionnaire, and health- and fecal incontinence-related QoL. Assessments were conducted at baseline before randomization, at three months and one-year follow-ups.
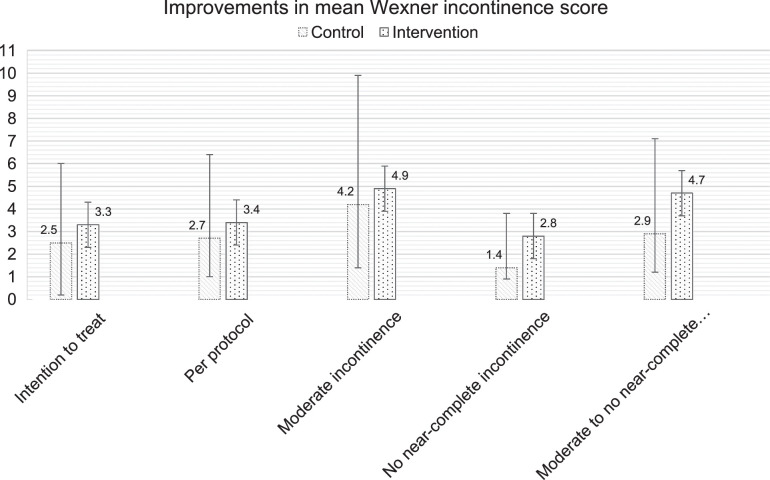
Results: A total of 86 patients were included (PFR: n=40, control: n=46). After one year, PFR did not significantly improve Wexner incontinence scores (PFR: -3.33, 95% CI -4.41 to -2.26, control: -2.54, 95% CI -3.54 to -1.54, P=0.30). Similar to the three-month follow-up, patients without near-complete incontinence at baseline showed sustained improvement in fecal incontinence (PFR: -2.82, 95% CI -3.86 to -1.76, control: -1.43, 95% CI -2.36 to -0.50, P=0.06). Significant improvement was reported in the FIQL domains Lifestyle (PFR: 0.51, control: -0.13, P=0.03) and Coping and Behavior (PFR: 0.40, control: -0.24, P=0.01).
Conclusion: At one-year follow-up, no significant differences were found in fecal incontinence scores; however, PFR was associated with improved fecal incontinence related QoL compared to usual care.
Copyright © 2024 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflict of interest statement: The authors report no conflicts of interest.
Figures

References
-
- van Heinsbergen M, Van der Heijden JAG, Stassen LP, et al. The low anterior resection syndrome in a reference population: prevalence and predictive factors in the Netherlands. Colorectal Dis. 2020;22:46–52. - PubMed
-
- Emmertsen KJ, Laurberg S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg. 2012;255:922–928. - PubMed
-
- Hassan I, Cima RR. Quality of life after rectal resection and multimodality therapy. J Surg Oncol. 2007;96:684–692. - PubMed
-
- Pucciani F. A review on functional results of sphincter-saving surgery for rectal cancer: the anterior resection syndrome. Updates Surg. 2013;65:257–263. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
