

Lesions hyper- to isointense to surrounding liver in the hepatobiliary phase of gadoxetic acid-enhanced MRI
- PMID: 38900280
- PMCID: PMC11557620
- DOI: 10.1007/s00330-024-10829-x
Lesions hyper- to isointense to surrounding liver in the hepatobiliary phase of gadoxetic acid-enhanced MRI
Abstract
Objectives: Hyper- or isointensity in the hepatobiliary phase (HBP) of gadoxetic acid-enhanced MRI has high specificity for focal nodular hyperplasia (FNH) but may be present in hepatocellular adenoma and carcinoma (HCA/HCC). This study aimed to identify imaging characteristics differentiating FNH and HCA/HCC.
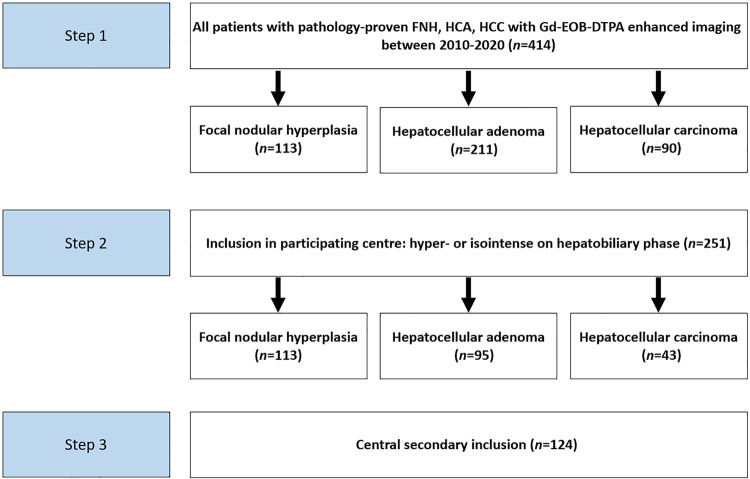
Materials and methods: This multicenter retrospective cohort study included patients with pathology-proven FNH or HCA/HCC, hyper-/isointense in the HBP of gadoxetic acid-enhanced MRI between 2010 and 2020. Diagnostic performance of imaging characteristics for the differentiation between FNH and HCA/HCC were reported. Univariable analyses, multivariable logistic regression analyses, and classification and regression tree (CART) analyses were conducted. Sensitivity analyses evaluated imaging characteristics of B-catenin-activated HCA.
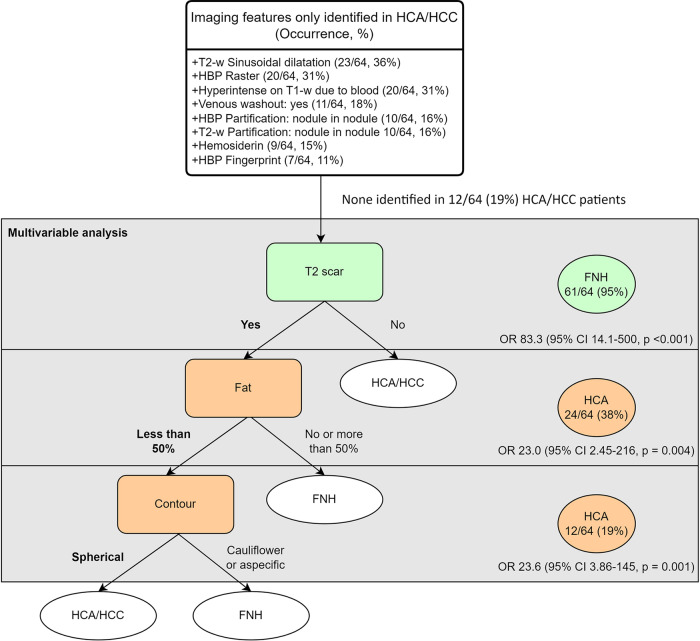
Results: In total, 124 patients (mean age 40 years, standard deviation 10 years, 108 female) with 128 hyper-/isointense lesions were included. Pathology diagnoses were FNH and HCA/HCC in 64 lesions (50%) and HCA/HCC in 64 lesions (50%). Imaging characteristics observed exclusively in HCA/HCC were raster and atoll fingerprint patterns in the HBP, sinusoidal dilatation on T2-w, hemosiderin, T1-w in-phase hyperintensity, venous washout, and nodule-in-nodule partification in the HBP and T2-w. Multivariable logistic regression and CART additionally found a T2-w scar indicating FNH, less than 50% fat, and a spherical contour indicating HCA/HCC. In our selected cohort, 14/48 (29%) of HCA were B-catenin activated, most (13/14) showed extensive hyper-/isointensity, and some had a T2-w scar (4/14, 29%).
Conclusion: If the aforementioned characteristics typical for HCA/HCC are encountered in lesions extensively hyper- to isointense, further investigation may be warranted to exclude B-catenin-activated HCA.
Clinical relevance: Hyper- or isointensity in the HBP of gadoxetic acid-enhanced MRI is specific for FNH, but HCA/HCC can also exhibit this feature. Therefore, we described imaging patterns to differentiate these entities.
Key points: FNH and HCA/HCC have similar HBP intensities but have different malignant potentials. Six imaging patterns exclusive to HCA/HCC were identified in this lesion population. These features in liver lesions hyper- to isointense in the HBP warrant further evaluation.
Keywords: Focal nodular hyperplasia; Gadolinium DTPA; Hepatocellular carcinoma; Liver cell adenoma; Magnetic resonance imaging.
© 2024. The Author(s).
Conflict of interest statement
Figures
Comment in
-
Illuminating the shades of hyper- to isointense lesions in hepatobiliary phase imaging.Eur Radiol. 2024 Dec;34(12):7659-7660. doi: 10.1007/s00330-024-10894-2. Epub 2024 Jul 9. Eur Radiol. 2024. PMID: 38981895 No abstract available.
References
-
- Fujita N, Nishie A, Asayama Y et al (2020) Hyperintense liver masses at hepatobiliary phase gadoxetic acid-enhanced MRI: imaging appearances and clinical importance. Radiographics 40:72–94. 10.1148/rg.2020190037 - PubMed
-
- European Association for the Study of the Liver (2016) EASL clinical practice guidelines on the management of benign liver tumours. J Hepatol 65:386–398. 10.1016/j.jhep.2016.04.001 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
